You might also like
- Ecg CmuDocument34 pagesEcg CmuArslan KhanNo ratings yet
- ECG1Document67 pagesECG1Farhan RosliNo ratings yet
- The Electrocardiogram: Normal Conduction PathwayDocument16 pagesThe Electrocardiogram: Normal Conduction PathwayFourth YearNo ratings yet
- MUCLecture 2021 1292271Document34 pagesMUCLecture 2021 1292271Kouka MahfoudiNo ratings yet
- ECG Interpretation GuideDocument69 pagesECG Interpretation GuideRohini RaiNo ratings yet
- Electrical Activity of The HeartDocument156 pagesElectrical Activity of The HeartNIRANJANA SHALININo ratings yet
- Ecg 1Document198 pagesEcg 1hibaNo ratings yet
- ECG Guide: Understanding Heart Rhythms & EKG TestDocument10 pagesECG Guide: Understanding Heart Rhythms & EKG TestSilver Villota Magday Jr.No ratings yet
- ECG Complete LectureDocument33 pagesECG Complete LectureDr. SUVA NATHNo ratings yet
- DrAbnet ECG - BasicsDocument99 pagesDrAbnet ECG - BasicsAbnet WondimuNo ratings yet
- Electrocardiography ECGDocument60 pagesElectrocardiography ECGSalman KhanNo ratings yet
- Electro Cardiogram & DysrythmiasDocument40 pagesElectro Cardiogram & DysrythmiasshobharamkrishnaNo ratings yet
- Lab Exercise 5 PDFDocument50 pagesLab Exercise 5 PDFE1- Villapaz, Aiemarie R. (Aie)No ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- ECG Lecture 1 by Dr. RoomiDocument18 pagesECG Lecture 1 by Dr. RoomiMudassar Roomi100% (3)
- How To Read An EcgDocument86 pagesHow To Read An EcgmajdNo ratings yet
- Electrocardiogra (M) PhyDocument26 pagesElectrocardiogra (M) PhyyansliyaNo ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- A Noob's Guide to ECG InterpretationDocument103 pagesA Noob's Guide to ECG InterpretationTeodorescu Claudia GabrielaNo ratings yet
- EKG 12 Lead GuideDocument59 pagesEKG 12 Lead GuideM Lukman HakimNo ratings yet
- Lecture On Basics of ECG For 1st Year MBBS by Dr. RoomiDocument28 pagesLecture On Basics of ECG For 1st Year MBBS by Dr. RoomiMudassar Roomi100% (3)
- Ecg Interpretation: Gowtham Krishna JDocument60 pagesEcg Interpretation: Gowtham Krishna JGowtham KrishnaNo ratings yet
- Mechanical and Electrical Events of The Cardiac CycleDocument39 pagesMechanical and Electrical Events of The Cardiac CyclebhatsindhoorNo ratings yet
- Conduction and EcgDocument32 pagesConduction and EcgRadijska Postaja KoprivnicaNo ratings yet
- Ecg BSTDocument204 pagesEcg BSTAnusha Verghese100% (1)
- ELEKTROKARDIOGRAFI Ridwan 2018Document90 pagesELEKTROKARDIOGRAFI Ridwan 2018YogaNo ratings yet
- ECG BasicsDocument82 pagesECG BasicsMaza AmfoterikNo ratings yet
- ECGDocument44 pagesECGJay ItaliyaNo ratings yet
- Basic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNDocument34 pagesBasic Ecg Interpretation and Arrhythmia Recognition By: Ma. Victoria E. Martinez Er - RNMavic Martinez BuntalesNo ratings yet
- ECG Interpretation: Prepared byDocument16 pagesECG Interpretation: Prepared bypipoahmed51No ratings yet
- ECG Basics Module-1Document127 pagesECG Basics Module-1manyusinghNo ratings yet
- DYSRHYTMIASDocument16 pagesDYSRHYTMIASVictor StevenNo ratings yet
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- Cardiac Output by N.Anisha MPT OrthoDocument53 pagesCardiac Output by N.Anisha MPT OrthoAnisha NallasamyNo ratings yet
- Basis of ECG and Intro To ECG InterpretationDocument10 pagesBasis of ECG and Intro To ECG InterpretationKristin SmithNo ratings yet
- BASIC ECG CKKDocument79 pagesBASIC ECG CKKAlexzander BrendonNo ratings yet
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- Normal ECGDocument63 pagesNormal ECGMohd Johari Mohd ShafuwanNo ratings yet
- ElectrocardiogramDocument3 pagesElectrocardiogramgaratoh099No ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (1)
- ECG: A Noob's Guide to Understanding ElectrocardiographyDocument103 pagesECG: A Noob's Guide to Understanding ElectrocardiographyGhaidaa Sadeq100% (1)
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Electrocardiogram (ECG) : This Is The Lecture No. 4Document51 pagesElectrocardiogram (ECG) : This Is The Lecture No. 4Aboodsha ShNo ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Electrocardiogram (ECG)Document53 pagesElectrocardiogram (ECG)eric100% (1)
- ECG Guide: Everything You Need to Know About ElectrocardiogramsDocument72 pagesECG Guide: Everything You Need to Know About ElectrocardiogramsGaras AnnaBerniceNo ratings yet
- Electrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHDocument42 pagesElectrocardiogram: Edit By: Pea Vuthy Edited From: CMMC/JHNorPhea - នភាNo ratings yet
- ECG TeachingDocument5 pagesECG Teachingmeyyappan nachiappanNo ratings yet
- Depolarization and RepolarizationDocument3 pagesDepolarization and Repolarizationمحمد سعد طه احمدNo ratings yet
- Normal ECG Waveforms and Intervals ExplainedDocument26 pagesNormal ECG Waveforms and Intervals ExplainedJan Christian AramburoNo ratings yet
- Ecg ProcedureDocument5 pagesEcg ProcedureLungu AdrianNo ratings yet
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Quick Healthcare Stencil: SketchDocument2 pagesQuick Healthcare Stencil: SketchNafiz Hannan NabilNo ratings yet
- Adverse Drug Reactions in A ComplementaryDocument8 pagesAdverse Drug Reactions in A Complementaryrr48843No ratings yet
- VPN Risk Report Cybersecurity InsidersDocument20 pagesVPN Risk Report Cybersecurity InsidersMaria PerezNo ratings yet
- Homework No1. Kenner Pérez TurizoDocument6 pagesHomework No1. Kenner Pérez TurizoKenner PérezNo ratings yet
- TM 5-5031 HOLLINGSWORTH GENERATORS CE-51-DC AND DC - WK2 MODELS, 1953Document16 pagesTM 5-5031 HOLLINGSWORTH GENERATORS CE-51-DC AND DC - WK2 MODELS, 1953Advocate100% (1)
- Hepatobiliary Surgery BlumgartDocument301 pagesHepatobiliary Surgery Blumgartaejazahsan100% (7)
- CeramicsDocument39 pagesCeramicsD4-dc1 Kelas100% (1)
- Wheatstone Bridge Circuit and Theory of OperationDocument7 pagesWheatstone Bridge Circuit and Theory of OperationAminullah SharifNo ratings yet
- Dermatitis Venenata Donald UDocument5 pagesDermatitis Venenata Donald UIndahPertiwiNo ratings yet
- CompReg 13SEPTEMBER2023Document2,725 pagesCompReg 13SEPTEMBER2023syed pashaNo ratings yet
- 28 GHZ Millimeter Wave Cellular Communication Measurements For Reflection and Penetration Loss in and Around Buildings in New York CityDocument5 pages28 GHZ Millimeter Wave Cellular Communication Measurements For Reflection and Penetration Loss in and Around Buildings in New York CityJunyi LiNo ratings yet
- Rate of Change: Example 1 Determine All The Points Where The Following Function Is Not ChangingDocument5 pagesRate of Change: Example 1 Determine All The Points Where The Following Function Is Not ChangingKishamarie C. TabadaNo ratings yet
- A Light Sculling Training Boat PDFDocument8 pagesA Light Sculling Training Boat PDFLuis BraulinoNo ratings yet
- Ammonium Nitrophosphate Production ProcessDocument133 pagesAmmonium Nitrophosphate Production ProcessHit Busa100% (1)
- Cu Unjieng V MabalacatDocument6 pagesCu Unjieng V MabalacatMp CasNo ratings yet
- Cylinder Liner W32Document1 pageCylinder Liner W32Poma100% (1)
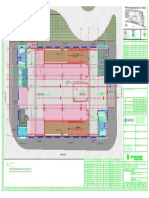
- Key plan and area statement comparison for multi-level car park (MLCPDocument1 pageKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYANo ratings yet
- Louise Bedford Trading InsightsDocument80 pagesLouise Bedford Trading Insightsartendu100% (3)
- Chapter 3 Theoretical ConsiderationsDocument8 pagesChapter 3 Theoretical Considerationsapi-3696675No ratings yet
- Particulars Unit BOQ NO. BOQ QTY: Bill of Quantity Bill of QuantityDocument8 pagesParticulars Unit BOQ NO. BOQ QTY: Bill of Quantity Bill of QuantityAbbasNo ratings yet
- Physics Chapter on Motion and Force EquationsDocument2 pagesPhysics Chapter on Motion and Force EquationsMalikXufyanNo ratings yet
- GCAF Online Inspector Practice ExamDocument5 pagesGCAF Online Inspector Practice Examcamwills2100% (1)
- 3RT10241AB00 Datasheet enDocument7 pages3RT10241AB00 Datasheet enanon_92005543No ratings yet
- 5 Hunger of The PineDocument39 pages5 Hunger of The PinedraconeitNo ratings yet
- FELDocument71 pagesFELElimel Rome Rico100% (4)
- O Bio Summarize Notes For RevisionDocument31 pagesO Bio Summarize Notes For RevisionAfifa AmerNo ratings yet
- Boosting BARMM Infrastructure for Socio-Economic GrowthDocument46 pagesBoosting BARMM Infrastructure for Socio-Economic GrowthEduardo LongakitNo ratings yet
- Ahmed (2018)Document9 pagesAhmed (2018)zrancourttremblayNo ratings yet
- Java Material 1Document84 pagesJava Material 1tvktrueNo ratings yet
- Conflict Analysis Tools PDFDocument12 pagesConflict Analysis Tools PDFApeuDerrop0% (1)