You might also like
- The Brigham Intensive Review of Internal Medicine Q&A Companion, 2eDocument227 pagesThe Brigham Intensive Review of Internal Medicine Q&A Companion, 2eMalueth Angui100% (4)
- Some Biochem MnemonicsDocument8 pagesSome Biochem MnemonicsMikey PalominoNo ratings yet
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 pagesCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaNo ratings yet
- Eric Berg CVDocument6 pagesEric Berg CVHaralambicNo ratings yet
- Guidelines For The Use of Fresh-Frozen Plasma, Cryoprecipitate & CryosupernantDocument18 pagesGuidelines For The Use of Fresh-Frozen Plasma, Cryoprecipitate & CryosupernantAymen OmerNo ratings yet
- CoagulopathyDocument121 pagesCoagulopathyMegat Mohd Azman AdzmiNo ratings yet
- CUTANEOUS VasculitisDocument78 pagesCUTANEOUS VasculitisDeepshikhaKhannaNo ratings yet
- Disseminated Intravascular Coagulation: Treat The Cause, Not The Lab ValuesDocument9 pagesDisseminated Intravascular Coagulation: Treat The Cause, Not The Lab Valuesboris_beroizaNo ratings yet
- Review of Literature on Rabies Prevention and ControlDocument24 pagesReview of Literature on Rabies Prevention and ControlBeah Claudette AbundoNo ratings yet
- 2014 Final Paediatric Exam (تم الحفظ تلقائيًا)Document258 pages2014 Final Paediatric Exam (تم الحفظ تلقائيًا)wea xcz100% (4)
- Graft vs. Host Disease (GVHD) : Abdullah 3 Year MBBS Batch#15 Roll#22Document37 pagesGraft vs. Host Disease (GVHD) : Abdullah 3 Year MBBS Batch#15 Roll#22Muhammad AbdullahNo ratings yet
- Acute Lymphoblastic Leukemia Incidence, Epidemiology, Etiology and ClassificationDocument19 pagesAcute Lymphoblastic Leukemia Incidence, Epidemiology, Etiology and ClassificationNeng AyuRati50% (2)
- A-Gvhd M.saeedDocument20 pagesA-Gvhd M.saeedaymenNo ratings yet
- VOD - SOS in HSCTDocument25 pagesVOD - SOS in HSCTKim-Thinh Nguyen ThiNo ratings yet
- Clinical Manifestations and Diagnosis of Chronic Graft-Versus-host Disease - UpToDateDocument39 pagesClinical Manifestations and Diagnosis of Chronic Graft-Versus-host Disease - UpToDateSergiu MoraruNo ratings yet
- Treatment of Chronic Graft-Versus-Host Disease - UpToDateDocument23 pagesTreatment of Chronic Graft-Versus-Host Disease - UpToDatemihaela popescuNo ratings yet
- All Aml NCCN 2023 HamidahDocument45 pagesAll Aml NCCN 2023 HamidahPPDS IPD ULMNo ratings yet
- Chronic Lymphocytic Leukemia: 1) EtiologyDocument6 pagesChronic Lymphocytic Leukemia: 1) EtiologyMarcoNo ratings yet
- Benign Hematology Conference 9/28/2021: Ghazal KangoDocument25 pagesBenign Hematology Conference 9/28/2021: Ghazal KangoGhazal KangoNo ratings yet
- Bleeding PPT 4Document23 pagesBleeding PPT 4Nidya PutriNo ratings yet
- 1 - Hodgkin's LymphomaDocument12 pages1 - Hodgkin's LymphomaDiana MitreaNo ratings yet
- Febrile NeutropeniaDocument35 pagesFebrile NeutropeniaYogesh ShindeNo ratings yet
- If HP Cancer Guide BMT ManualDocument363 pagesIf HP Cancer Guide BMT ManualZardar KNo ratings yet
- Pathogenesis of Graft-Versus-Host Disease (GVHD) - UpToDateDocument12 pagesPathogenesis of Graft-Versus-Host Disease (GVHD) - UpToDatemihaela popescuNo ratings yet
- GVHDDocument35 pagesGVHDSaad KhanNo ratings yet
- Graft Versus Host Disease ExplainedDocument14 pagesGraft Versus Host Disease ExplainedBoutheyna MahmoudNo ratings yet
- Transfusion ReactionsDocument36 pagesTransfusion Reactionsmarky203No ratings yet
- Acute LeukemiasDocument48 pagesAcute LeukemiaslaibaNo ratings yet
- HIV Neurology: Graeme MeintjesDocument75 pagesHIV Neurology: Graeme MeintjesPrincess MiraNo ratings yet
- Anticoagulation On COVID-19 Associated Coagulopathy 2Document41 pagesAnticoagulation On COVID-19 Associated Coagulopathy 2ihsan mnNo ratings yet
- MiscDocument29 pagesMiscsam2000samNo ratings yet
- Hodgkin Lymphoma KlapperDocument17 pagesHodgkin Lymphoma KlapperAthika RodhyaNo ratings yet
- CCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷Document6 pagesCCCCCCCCCCCCCCCCCCCCCCCCCC C C ÷shaikameermalikNo ratings yet
- Graft vs. Host Disease ExplainedDocument35 pagesGraft vs. Host Disease ExplainedSaad KhanNo ratings yet
- Gestational Trophoblastic Disease Pt2Document75 pagesGestational Trophoblastic Disease Pt2yurie_ameliaNo ratings yet
- Ojim 2016091213324550Document10 pagesOjim 2016091213324550rianmg21No ratings yet
- Dermatologic extrahepatic manifestations of Hepatitis CDocument7 pagesDermatologic extrahepatic manifestations of Hepatitis Cgwyneth.green.512No ratings yet
- Biological and Targeted Therapy VILis The Fourth Treatment ModalityDocument7 pagesBiological and Targeted Therapy VILis The Fourth Treatment ModalityAlan CJNo ratings yet
- Acute Rejection DR Sihir GangDocument38 pagesAcute Rejection DR Sihir GangwandaNo ratings yet
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDocument41 pagesHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriNo ratings yet
- Blood and Marrow Transplant:: Resident Education Lecture SeriesDocument30 pagesBlood and Marrow Transplant:: Resident Education Lecture SeriesAparna KinginiNo ratings yet
- Venous Thromboembolism in MalignancyDocument3 pagesVenous Thromboembolism in MalignancyAzmi FarhadiNo ratings yet
- HIV/AIDS Kaposi's Sarcoma Treatment GuideDocument55 pagesHIV/AIDS Kaposi's Sarcoma Treatment GuideAndrei CluNo ratings yet
- CMV SEMINARDocument38 pagesCMV SEMINARsaraabolghasemi1No ratings yet
- Location Gold Standard Current Practice: Thrombophilia Teaching Points10/19/2005 (JGP)Document2 pagesLocation Gold Standard Current Practice: Thrombophilia Teaching Points10/19/2005 (JGP)aymenNo ratings yet
- Graft Versus Host Disease..Document2 pagesGraft Versus Host Disease..Sakawath HosainNo ratings yet
- VTE Prophylaxis in The Hospital: Johan KurniandaDocument35 pagesVTE Prophylaxis in The Hospital: Johan KurniandaadystiNo ratings yet
- Chronic Lymphocytic LeukemiaDocument43 pagesChronic Lymphocytic LeukemialaibaNo ratings yet
- Pathology of Extra Hepatic HCV ManifestationsDocument21 pagesPathology of Extra Hepatic HCV Manifestationsostaz2000No ratings yet
- Chapter 15+17 Hemorrhagic Disease & Thrombocytopenic PurpuraDocument20 pagesChapter 15+17 Hemorrhagic Disease & Thrombocytopenic PurpuraFathimathNo ratings yet
- Chapter 15+17 Hemorrhagic Disease & Thrombocytopenic PurpuraDocument20 pagesChapter 15+17 Hemorrhagic Disease & Thrombocytopenic PurpuraFathimathNo ratings yet
- BLEEDING DISORDERS: CLINICAL ASPECTS AND MANAGEMENTDocument69 pagesBLEEDING DISORDERS: CLINICAL ASPECTS AND MANAGEMENTAndrew Leonardo Panjaitan100% (1)
- Hepatology MRCP1Document87 pagesHepatology MRCP1Raouf Ra'fat SolimanNo ratings yet
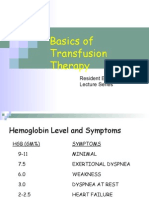
- Basics of Transfusion TherapyDocument43 pagesBasics of Transfusion TherapyMuhammad Afyudin DjumhuriNo ratings yet
- Oct 4 0900 - W15 ZedDocument58 pagesOct 4 0900 - W15 Zedjames lxNo ratings yet
- Acute Lymphoblastic Leukemia: Differential DiagnosisDocument6 pagesAcute Lymphoblastic Leukemia: Differential DiagnosisIma OhwNo ratings yet
- Essential Thrombocythemia: Risk Factors, Mutations, ManagementDocument8 pagesEssential Thrombocythemia: Risk Factors, Mutations, ManagementHana MelissaNo ratings yet
- TB and HIV Co-Infection: A Guide to Diagnosing and Treating Opportunistic InfectionsDocument88 pagesTB and HIV Co-Infection: A Guide to Diagnosing and Treating Opportunistic InfectionsovidiuroscaNo ratings yet
- Renal Transplantation An OverviewDocument58 pagesRenal Transplantation An OverviewSony's TechNo ratings yet
- Relapsed Refractory AMLDocument114 pagesRelapsed Refractory AMLKishoreChandraKoradaNo ratings yet
- Cervix Cancer Treatment and Staging ReviewDocument11 pagesCervix Cancer Treatment and Staging ReviewDiana MitreaNo ratings yet
- Thrombocytopenia Sarah WalterDocument49 pagesThrombocytopenia Sarah WalterSupicha VichaiditNo ratings yet
- Course 3 Liver and Heart Transplantation PDFDocument22 pagesCourse 3 Liver and Heart Transplantation PDFVladimir PetreNo ratings yet
- A 1Document5 pagesA 1cikobernicaNo ratings yet
- Managing sickle cell anemiaDocument41 pagesManaging sickle cell anemiaRommel Montero RicioNo ratings yet
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
- Estimation of Impedance Platelet Count A PDFDocument4 pagesEstimation of Impedance Platelet Count A PDFAymen OmerNo ratings yet
- Bacterial Contamination.: Prepared By: Raitha R Suleiman Alexandria University 2018Document13 pagesBacterial Contamination.: Prepared By: Raitha R Suleiman Alexandria University 2018Aymen OmerNo ratings yet
- Seek Crit Care 26 Sample NewDocument6 pagesSeek Crit Care 26 Sample NewAymen OmerNo ratings yet
- FigureDocument1 pageFigureAymen OmerNo ratings yet
- Normal Ranges Core HaematologyDocument1 pageNormal Ranges Core HaematologyAymen OmerNo ratings yet
- A Guideline For The Diagnosis and Management of Polycythaemia VeraDocument23 pagesA Guideline For The Diagnosis and Management of Polycythaemia VeraAymen OmerNo ratings yet
- Chronic GVHD Symptom ScaleDocument5 pagesChronic GVHD Symptom ScaleAymen OmerNo ratings yet
- Transplantation &: Tissue RejectionDocument15 pagesTransplantation &: Tissue RejectionAymen OmerNo ratings yet
- Testicular Feminization Syndrome TFM: Ruslan Bayramov .MD Medical Genetics Department Erciyes UniversityDocument25 pagesTesticular Feminization Syndrome TFM: Ruslan Bayramov .MD Medical Genetics Department Erciyes UniversityAymen OmerNo ratings yet
- Haploidentical Stem Cell Transplant: Zeina Al-Mansour, MDDocument22 pagesHaploidentical Stem Cell Transplant: Zeina Al-Mansour, MDAymen OmerNo ratings yet
- Diagnosis and Management of Polycythaemia VeraDocument16 pagesDiagnosis and Management of Polycythaemia VeraAymen OmerNo ratings yet
- Varient CML BCR-ABL PositiveDocument11 pagesVarient CML BCR-ABL PositiveAymen OmerNo ratings yet
- 9123633Document99 pages9123633Aymen OmerNo ratings yet
- Biochemistrypresentation Copy 150905173417 Lva1 App6892Document20 pagesBiochemistrypresentation Copy 150905173417 Lva1 App6892Dawlat SalamaNo ratings yet
- Aml 1Document2 pagesAml 1Aymen OmerNo ratings yet
- Alternatives 2006Document7 pagesAlternatives 2006Aymen OmerNo ratings yet
- Hypercalcaemia and Hypercalciuria: JamieDocument11 pagesHypercalcaemia and Hypercalciuria: JamieAymen OmerNo ratings yet
- Basic Epidemiologic and Biostatistical Terminology ForDocument15 pagesBasic Epidemiologic and Biostatistical Terminology ForAymen OmerNo ratings yet
- Hepatitsppt 151223190415Document26 pagesHepatitsppt 151223190415Aymen OmerNo ratings yet
- Hepatitis C Virus: Section: 3Document43 pagesHepatitis C Virus: Section: 3Aymen OmerNo ratings yet
- 4-27 8am Halder - Cutaneous Manif. of Diseases2Document12 pages4-27 8am Halder - Cutaneous Manif. of Diseases2Aymen OmerNo ratings yet
- Extrinsic PathwayDocument1 pageExtrinsic PathwayAymen OmerNo ratings yet
- Hepatorenal SyndromeDocument4 pagesHepatorenal SyndromeAymen OmerNo ratings yet
- Surviving 4th Year MedicineDocument64 pagesSurviving 4th Year MedicineAymen OmerNo ratings yet
- Study of The Pattern of Chest Diseases Including Tuberculosis in Qena Chest HospitalDocument10 pagesStudy of The Pattern of Chest Diseases Including Tuberculosis in Qena Chest HospitalAymen OmerNo ratings yet
- Structure of The Protocol 2Document10 pagesStructure of The Protocol 2Aymen OmerNo ratings yet
- DUODENAL PROCEDUREDocument5 pagesDUODENAL PROCEDUREeka nurjanahNo ratings yet
- Obstetrics and GynacologyDocument14 pagesObstetrics and GynacologykalkidanNo ratings yet
- KenyaEMR v17.3.1 Release Notes SummaryDocument3 pagesKenyaEMR v17.3.1 Release Notes SummaryMigori Art DataNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Experiment #2 - Unit TaskDocument2 pagesExperiment #2 - Unit TaskKagami TaigaNo ratings yet
- Mgi Presentation - ReyDocument65 pagesMgi Presentation - ReyCharlot Jade Paderes67% (3)
- PATIENT INFORMATION - New App System - WebsiteDocument2 pagesPATIENT INFORMATION - New App System - WebsiteA M P KumarNo ratings yet
- Minimum Inhibitory ConcentrationDocument7 pagesMinimum Inhibitory ConcentrationToshio HamazakiNo ratings yet
- Nursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDocument5 pagesNursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDr-Marudhar MarudharNo ratings yet
- ICU Accomplishment Report and Improvement PlanDocument5 pagesICU Accomplishment Report and Improvement PlanMikhaelEarlSantosTacordaNo ratings yet
- Medication To Manage Abortion and MiscarriageDocument8 pagesMedication To Manage Abortion and MiscarriageNisaNo ratings yet
- C-Section Guide: What to Expect with Cesarean DeliveryDocument3 pagesC-Section Guide: What to Expect with Cesarean DeliveryFEALABREPORTSNo ratings yet
- Infectiile Grave Extensive Ale Partilor MoiDocument49 pagesInfectiile Grave Extensive Ale Partilor MoiLoredana BoghezNo ratings yet
- Body's Battles (gnv64) PDFDocument96 pagesBody's Battles (gnv64) PDFameyparanjape100% (1)
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDocument8 pagesVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengNo ratings yet
- Necrotizing Soft Tissue Infections GuideDocument21 pagesNecrotizing Soft Tissue Infections GuideHen RyNo ratings yet
- Lesson 1Document20 pagesLesson 1Irish Jean AgsawayNo ratings yet
- Resume - Viroja Sweta For PortfolioDocument1 pageResume - Viroja Sweta For Portfolioapi-608195339No ratings yet
- Amavatha & VathasonithaDocument125 pagesAmavatha & VathasonithaCicil AbrahamNo ratings yet
- Conscious Sedation PaediatricsDocument44 pagesConscious Sedation PaediatricsReeta TaxakNo ratings yet
- Femur and Pelvis Fracture (Trauma)Document20 pagesFemur and Pelvis Fracture (Trauma)Ree YahNo ratings yet
- MSUDDocument23 pagesMSUDDivya AjithNo ratings yet
- Hipertensi Portal Donny SandraDocument67 pagesHipertensi Portal Donny SandrabobyNo ratings yet
- Jomi 7657Document27 pagesJomi 7657casto.carpetasmiaNo ratings yet
- Not Eligible As No Experience of Teaching and ResearchDocument5 pagesNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNo ratings yet
- PrimaquineDocument3 pagesPrimaquineVijayakumar NsNo ratings yet