You might also like
- Cherokee Herbal RemediesDocument292 pagesCherokee Herbal RemediesAlek Phabiovsky100% (2)
- Hydrogen Peroxide TherapyDocument0 pagesHydrogen Peroxide TherapyGetto Vocab100% (2)
- Lung Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandLung Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 2014 Body Code Client Information PDFDocument7 pages2014 Body Code Client Information PDFkrug100% (1)
- Respiratory gymnastics (Translated): Purification - Health - Strength - EnergyFrom EverandRespiratory gymnastics (Translated): Purification - Health - Strength - EnergyNo ratings yet
- Saudi Commission Manual Classifies Health PractitionersDocument38 pagesSaudi Commission Manual Classifies Health Practitionerstoplexil100% (1)
- Cardiovascular Physiology Case 9Document50 pagesCardiovascular Physiology Case 9Kim AcostaNo ratings yet
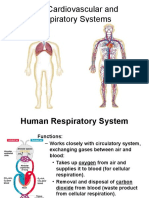
- The Human Cardiovascular and Respiratory SystemsDocument51 pagesThe Human Cardiovascular and Respiratory SystemsAlexi Nicole CastaloneNo ratings yet
- Case Study: Chronic BronchitisDocument9 pagesCase Study: Chronic BronchitisDivine ParagasNo ratings yet
- Case Study PneumoniaDocument13 pagesCase Study Pneumonialavparedes93% (44)
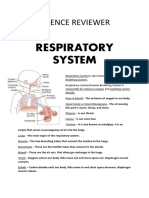
- Respiratory SystemDocument10 pagesRespiratory Systemapi-272862164No ratings yet
- Amyotrophic Lateral SclerosisDocument70 pagesAmyotrophic Lateral SclerosisLorenz Hernandez100% (1)
- Breath Taking: The Power, Fragility, and Future of Our Extraordinary LungsFrom EverandBreath Taking: The Power, Fragility, and Future of Our Extraordinary LungsRating: 3.5 out of 5 stars3.5/5 (5)
- Pulmonary EmbolismDocument21 pagesPulmonary EmbolismMadhu Bala100% (2)
- Sexually Transmitted InfectionsDocument110 pagesSexually Transmitted Infectionstummalapalli venkateswara raoNo ratings yet
- Cardiovascular and Respiratory SystemDocument51 pagesCardiovascular and Respiratory SystemKarel Mae SanoriaNo ratings yet
- Mental Health Term PaperDocument8 pagesMental Health Term Paperchememartinez29100% (2)
- Market IntegrationDocument33 pagesMarket Integrationchememartinez2986% (7)
- Viral Exanthems: Sahara Tuazan AbonawasDocument75 pagesViral Exanthems: Sahara Tuazan AbonawasMarlon Cenabre Turaja100% (1)
- Treatment of Diabetic Neuropathy - UpToDateDocument20 pagesTreatment of Diabetic Neuropathy - UpToDateKarina MilaréNo ratings yet
- Respiratory System AssessmentDocument13 pagesRespiratory System Assessmentavinash dhameriyaNo ratings yet
- Human Body SystemsDocument9 pagesHuman Body SystemsTiara Dwi PangestutiNo ratings yet
- Judgement and PripositionsDocument7 pagesJudgement and Pripositionschememartinez29No ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of Nursingcaloy10No ratings yet
- PneumoniaDocument43 pagesPneumoniaagnescabintoy100% (2)
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- Pneumonia PathoDocument38 pagesPneumonia PathoIvan Michael IcaoNo ratings yet
- UNIT 3.2 The Respiratory System and Digestive and Respiratory Related IllnessesDocument21 pagesUNIT 3.2 The Respiratory System and Digestive and Respiratory Related IllnessesCarlos FloresNo ratings yet
- Systems Module 12Document40 pagesSystems Module 12Richiel Angulo SungaNo ratings yet
- ScienceDocument14 pagesSciencesheanellerenzsantosNo ratings yet
- Cardiovascular and Respiratory SystemDocument44 pagesCardiovascular and Respiratory SystemKlaudette Collin PaynorNo ratings yet
- 7th Grade Biology Notes on Respiration and Gas ExchangeDocument6 pages7th Grade Biology Notes on Respiration and Gas ExchangeSahithi PNo ratings yet
- Respiratory System in Human BeingsDocument11 pagesRespiratory System in Human BeingsSarada KasyapNo ratings yet
- Resprn in Humns-KDBDocument52 pagesResprn in Humns-KDBKiranNo ratings yet
- Respiratory System Functions and AlterationsDocument15 pagesRespiratory System Functions and Alterationsfiel borataNo ratings yet
- Cardiovascular and Respiratory SystemDocument51 pagesCardiovascular and Respiratory Systemnarichu92No ratings yet
- Eals ReviewerDocument12 pagesEals ReviewerEms TeopeNo ratings yet
- Unit 1 - Respiration - Reference Material - Shared in GCDocument7 pagesUnit 1 - Respiration - Reference Material - Shared in GCTarunNo ratings yet
- Respiration: How Cells Convert EnergyDocument45 pagesRespiration: How Cells Convert EnergyMaleeha HumayunNo ratings yet
- Respiratory SystemDocument24 pagesRespiratory SystemIan GarciaNo ratings yet
- What Is Respiration?Document8 pagesWhat Is Respiration?Waleed Bin KhalidNo ratings yet
- Genbio2 RespirationDocument1 pageGenbio2 RespirationArvie Jane Mendoza DeTorresNo ratings yet
- Respiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemDocument31 pagesRespiratory System: Agatha Babyet A. Alabata, Bsn-Iii StemJay VillasotoNo ratings yet
- The Respiratory System of Pigs Anatomy and FunctionDocument16 pagesThe Respiratory System of Pigs Anatomy and FunctionKrisi KehayovaNo ratings yet
- Respiratory SystemDocument2 pagesRespiratory SystemDearly Niña OsinsaoNo ratings yet
- ReviewerDocument10 pagesReviewerMaybelyn Rivera PagkatotohanNo ratings yet
- IGCSE Edexcel Biology RevisionDocument7 pagesIGCSE Edexcel Biology RevisionKonrad HuiNo ratings yet
- The Respiratory System-11 By:-Dr. Hazim AL-RawiDocument12 pagesThe Respiratory System-11 By:-Dr. Hazim AL-RawiDrAli Al-FendiNo ratings yet
- Now Get From Our Live Expert On Rea Ltime Basis Join Us and Get Homework HelpDocument17 pagesNow Get From Our Live Expert On Rea Ltime Basis Join Us and Get Homework HelplicservernoidaNo ratings yet
- Circulatory System & Respiration HODocument7 pagesCirculatory System & Respiration HODina Ayudan CortezNo ratings yet
- Chapter 1 - Respiratory and Circulatory Systems Working With The Other Organ SystemsDocument60 pagesChapter 1 - Respiratory and Circulatory Systems Working With The Other Organ SystemsPatricia Sofia DizonNo ratings yet
- Laporan Tutorial Blok 3.1: Disusun Oleh: Kelompok 2B Anggota KelompokDocument14 pagesLaporan Tutorial Blok 3.1: Disusun Oleh: Kelompok 2B Anggota KelompokrezaNo ratings yet
- 1r3ntvbfve - Ipa Kelas 8 Bab 9Document19 pages1r3ntvbfve - Ipa Kelas 8 Bab 9aulyamaltha.2008No ratings yet
- POINTERS-SCIENCE Grade 9 Quarter 1Document7 pagesPOINTERS-SCIENCE Grade 9 Quarter 1Lunyl DelloNo ratings yet
- Case Study PneumoniaDocument14 pagesCase Study PneumoniaDOni CorleoneNo ratings yet
- Respiratory Failure S/T HCAPDocument50 pagesRespiratory Failure S/T HCAPElaine Jean UayanNo ratings yet
- Respiratory System OverviewDocument4 pagesRespiratory System Overviewbunso padillaNo ratings yet
- Respiratory and Circulatory SystemDocument7 pagesRespiratory and Circulatory SystemElle MateoNo ratings yet
- Lymphatics and Respiratory SystemDocument67 pagesLymphatics and Respiratory Systemnursereview100% (2)
- Respiratory and Circulatory Systems ReviewDocument6 pagesRespiratory and Circulatory Systems ReviewRish NicoleNo ratings yet
- Students' Guide to PneumoniaDocument15 pagesStudents' Guide to PneumoniaArgenic BernzNo ratings yet
- Pharmd - 1Y - 1.1 - Human Anatomy PhysiologyDocument4 pagesPharmd - 1Y - 1.1 - Human Anatomy PhysiologySinger Rahul SharmaNo ratings yet
- Gen Bio ReviewerDocument5 pagesGen Bio ReviewercurtaranasNo ratings yet
- Respiratory SystemDocument43 pagesRespiratory SystemMaxxdlc 16No ratings yet
- All About RespiratoryDocument69 pagesAll About RespiratoryMarcellina Awing100% (1)
- Science 9 1st Quarter ReviewerDocument13 pagesScience 9 1st Quarter ReviewerFatima ShaenaNo ratings yet
- Deciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineFrom EverandDeciphering nCoV19, Quest for Cure, Prophylaxis, and VaccineNo ratings yet
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksFrom EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNo ratings yet
- Islamic Architecture: A Visual Guide to Key Styles and LandmarksDocument8 pagesIslamic Architecture: A Visual Guide to Key Styles and Landmarkschememartinez29No ratings yet
- Ma. Cherry Mhay S. MartinezDocument1 pageMa. Cherry Mhay S. Martinezchememartinez29No ratings yet
- Chapter 5 (Recommendation)Document5 pagesChapter 5 (Recommendation)chememartinez29No ratings yet
- ADPIEDocument1 pageADPIEchememartinez29No ratings yet
- Mama For PrintDocument6 pagesMama For Printchememartinez29No ratings yet
- Path o PhysiologyDocument3 pagesPath o Physiologychememartinez29No ratings yet
- Gerunds: Form and Use (#1), by Dennis OliverDocument3 pagesGerunds: Form and Use (#1), by Dennis Oliverchememartinez29No ratings yet
- ADPIE Model for Healthcare Assessment and TreatmentDocument32 pagesADPIE Model for Healthcare Assessment and Treatmentchememartinez29No ratings yet
- IntroductionDocument2 pagesIntroductionchememartinez29No ratings yet
- Female Reproductive SystemDocument9 pagesFemale Reproductive Systemchememartinez29No ratings yet
- European Rulers in The Age of AbsolutismDocument11 pagesEuropean Rulers in The Age of Absolutismchememartinez29No ratings yet
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Document5 pagesList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNo ratings yet
- Dental Anomalies II New PDFDocument34 pagesDental Anomalies II New PDFFranco Coco SartoriNo ratings yet
- Monnal t75 Air Liquide Ventilator PDFDocument10 pagesMonnal t75 Air Liquide Ventilator PDFFederico DonfrancescoNo ratings yet
- Drug Release Kinetics ModelsDocument7 pagesDrug Release Kinetics ModelsSajid Khan SadozaiNo ratings yet
- PRC FormDocument5 pagesPRC FormPamela DomingoNo ratings yet
- Physiotherapy in LeprosyDocument4 pagesPhysiotherapy in LeprosymichaelsophianNo ratings yet
- DR Wong Teck WeeipadDocument2 pagesDR Wong Teck Weeipadtwwong68No ratings yet
- Depression in Today - BioDocument5 pagesDepression in Today - Bioapi-272648963No ratings yet
- Blood Pressure Log 30Document2 pagesBlood Pressure Log 30Yousab KaldasNo ratings yet
- Dissertation Topics 2Document21 pagesDissertation Topics 2Apollo Institute of Hospital Administration100% (1)
- Pasteurized EggsDocument8 pagesPasteurized Eggsapi-202950260No ratings yet
- Pictorial Review of TI-RADS Scoring System for Thyroid Nodules (38 charactersDocument1 pagePictorial Review of TI-RADS Scoring System for Thyroid Nodules (38 charactersmanuel aguilarNo ratings yet
- Audit of Barangay Health Centers in PhilippinesDocument26 pagesAudit of Barangay Health Centers in PhilippineskenvysNo ratings yet
- Legumes - AnOverview PDFDocument6 pagesLegumes - AnOverview PDFMayuri JagtapNo ratings yet
- Hemorragic Post PartumDocument10 pagesHemorragic Post PartumJihan NurlailaNo ratings yet
- Wallen Et Al-2006-Australian Occupational Therapy JournalDocument1 pageWallen Et Al-2006-Australian Occupational Therapy Journal胡知行No ratings yet
- Iryu.4 Team - Medical.Dragon.E09.720p.Web ENGDocument45 pagesIryu.4 Team - Medical.Dragon.E09.720p.Web ENGcintoyNo ratings yet
- Adult Diarrhea GuideDocument15 pagesAdult Diarrhea GuideM.Reza ErlanggaNo ratings yet
- Older Adults Group PlanDocument31 pagesOlder Adults Group Planapi-316614503No ratings yet
- Kaloji Narayana Rao University Health Sciences College Allotment ListDocument79 pagesKaloji Narayana Rao University Health Sciences College Allotment ListVivek GuptaNo ratings yet
- Management of Perioperative ArrhythmiasDocument51 pagesManagement of Perioperative ArrhythmiasAbhishek LonikarNo ratings yet