You might also like
- The Sexaul SelfDocument15 pagesThe Sexaul SelfIan Michael BaangNo ratings yet
- 3 - Posterior TriangleDocument35 pages3 - Posterior TriangleMohammed Elfatih ElbadriNo ratings yet
- Female Sexual Response 2021Document34 pagesFemale Sexual Response 2021f3er3No ratings yet
- Clinical Review - Full PDFDocument6 pagesClinical Review - Full PDFDewi WulansariNo ratings yet
- Brain Wave Patterns Accompanying Changes Sleep Wakefulness HypnosisDocument10 pagesBrain Wave Patterns Accompanying Changes Sleep Wakefulness HypnosisjoskemorenikoONo ratings yet
- Chemistry and Pharmacology of Aphrodisiac Plants A ReviewDocument29 pagesChemistry and Pharmacology of Aphrodisiac Plants A ReviewEnema OJNo ratings yet
- Fournier's Gangrene EmergencyDocument4 pagesFournier's Gangrene EmergencyLalo ZaraloNo ratings yet
- Chapter+14 +sedative HynoticsDocument32 pagesChapter+14 +sedative Hynoticsudaysingh98100% (2)
- Post Radical Prostatectomy Penile Rehabilitation - AUA Update Series 2008Document8 pagesPost Radical Prostatectomy Penile Rehabilitation - AUA Update Series 2008Kevin ZornNo ratings yet
- General Principles of Laparoscopic Abdominal Surgery Pp2003Document18 pagesGeneral Principles of Laparoscopic Abdominal Surgery Pp2003jategaonkarpaNo ratings yet
- Lymphatic Drainage of The Head and Neck - AatifDocument6 pagesLymphatic Drainage of The Head and Neck - AatifAatif AnsariNo ratings yet
- Jurnal Fistolotomi Vs FistulektomiDocument8 pagesJurnal Fistolotomi Vs FistulektomiAndriati Nadhila100% (1)
- Amputation of The Penis: A.Venugopalan PG 212 LAS. 164Document14 pagesAmputation of The Penis: A.Venugopalan PG 212 LAS. 164Shayan JuttNo ratings yet
- Dr. Syahbudin - Complicated Perianal FistelDocument22 pagesDr. Syahbudin - Complicated Perianal FistelBlack DroneNo ratings yet
- 21 Neuro Urology LR2Document52 pages21 Neuro Urology LR2Retma Rosela NurkayantyNo ratings yet
- A Sole 16 12 14Document51 pagesA Sole 16 12 14Mariam AymanNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument29 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Physiology of Erection and EjaculationDocument1 pagePhysiology of Erection and EjaculationricohutabaratNo ratings yet
- Carcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, GotriDocument55 pagesCarcinoma of Penis: DR Hitesh Patel Associate Professor Surgery Department GMERS Medical College, Gotrihitesh3150% (1)
- Impotence (Erectile Dysfunction)Document28 pagesImpotence (Erectile Dysfunction)MwagaVumbi100% (1)
- What Is Brain Dead?Document1 pageWhat Is Brain Dead?The London Free Press100% (2)
- InfertilityDocument4 pagesInfertilitynica_ocampoNo ratings yet
- Inhalational AgentsDocument17 pagesInhalational Agentsanaeshkl100% (1)
- Anatomy PenisDocument7 pagesAnatomy PenisalexNo ratings yet
- Muscle of HandDocument15 pagesMuscle of HandcutbuleunNo ratings yet
- Uptake and Distribution of Volatile AnestheticsDocument22 pagesUptake and Distribution of Volatile AnestheticsSuresh Kumar100% (3)
- Chapter 6 Genital SystemDocument32 pagesChapter 6 Genital Systemapi-19916399No ratings yet
- Anatomy of Lower LimbDocument52 pagesAnatomy of Lower Limbdrkhan58No ratings yet
- Male Genitalia AbnormalitiesDocument25 pagesMale Genitalia AbnormalitiesClaudette Kyle CornelioNo ratings yet
- Medullary Sponge KidneyDocument3 pagesMedullary Sponge KidneyAmrAliTahaNo ratings yet
- Presented By, P.Jeyanthi, M.SC (N) I Year Apollo CONDocument67 pagesPresented By, P.Jeyanthi, M.SC (N) I Year Apollo CONPaul AndersonNo ratings yet
- Generalanaesthesia Drdhriti 111223120647 Phpapp01Document64 pagesGeneralanaesthesia Drdhriti 111223120647 Phpapp01Ridha Surya NugrahaNo ratings yet
- Low Back PainDocument34 pagesLow Back PainFAMED RESIDENTS CESMEDNo ratings yet
- Anatomy of ESophagusDocument28 pagesAnatomy of ESophagusAbdur RaqibNo ratings yet
- Post Operative Outcome by Different Surgical Procedures in Fistula in AnoDocument5 pagesPost Operative Outcome by Different Surgical Procedures in Fistula in AnoIJAR JOURNALNo ratings yet
- Sirkumsisi: Aji Setia UtamaDocument35 pagesSirkumsisi: Aji Setia UtamaAji Setia Utama100% (1)
- Anatomy of Forearm and Wrist - ppt1Document46 pagesAnatomy of Forearm and Wrist - ppt1Julian GordonNo ratings yet
- Cervical Plexus: Anatomy Presentation Submitted To: Ma'Am Nain Tara DPT 1 Proff (Morning)Document22 pagesCervical Plexus: Anatomy Presentation Submitted To: Ma'Am Nain Tara DPT 1 Proff (Morning)Hira Waseem100% (1)
- Sedatives and Hypnotics and Antianxiety: Wilson and Gisvold'sDocument41 pagesSedatives and Hypnotics and Antianxiety: Wilson and Gisvold'sRaushanKumarNo ratings yet
- Anatomy and Function of The Vagina and Pelvic MusclesDocument32 pagesAnatomy and Function of The Vagina and Pelvic MusclesleniucvasileNo ratings yet
- Comparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaDocument7 pagesComparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- Infratemporal Fossa: Dr. Prathyusha PG ENT Narayana Medical College NelloreDocument87 pagesInfratemporal Fossa: Dr. Prathyusha PG ENT Narayana Medical College NelloreSARAVANANNo ratings yet
- LG 1 (Half - The Salivary Glands)Document31 pagesLG 1 (Half - The Salivary Glands)allanNo ratings yet
- External & Internal Generative Organs OrgansDocument78 pagesExternal & Internal Generative Organs OrgansdeevoncNo ratings yet
- 2 Inguinal Region DiyaDocument31 pages2 Inguinal Region DiyaOmotosho DavidNo ratings yet
- Hernia FTDDocument71 pagesHernia FTDEmmanuel Papa AcquahNo ratings yet
- UntitledDocument84 pagesUntitledWardah AliNo ratings yet
- Maternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ADocument115 pagesMaternal Anatomy: Julao, Fritz Adrian C. Kho, Nicole Alexandra P. Lagmay, Paul Angelo ANicole Alexandra KhoNo ratings yet
- Perineal TearsDocument49 pagesPerineal TearsvisakhaNo ratings yet
- Sahitya Snigdha (Hernia Module)Document159 pagesSahitya Snigdha (Hernia Module)h9pkyd9dg9No ratings yet
- Anatomy of PharynxDocument35 pagesAnatomy of Pharynxadeyemieunice0000No ratings yet
- Anatomy and Physiology of Salivary GlandsDocument71 pagesAnatomy and Physiology of Salivary GlandsArun PadikkalveetilNo ratings yet
- Anatomy of Female Genital Tract - IiDocument44 pagesAnatomy of Female Genital Tract - Iigksah711No ratings yet
- Anal CanalDocument59 pagesAnal CanalLulu ShukkoorNo ratings yet
- Anatomy of GIT For PCII Students..Document106 pagesAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNo ratings yet
- General AnatomyDocument46 pagesGeneral AnatomyIhab IsmailNo ratings yet
- Maternal Anatomy External and Internal Generative OrgansDocument84 pagesMaternal Anatomy External and Internal Generative OrgansChristine HoNo ratings yet
- AnatomyDocument86 pagesAnatomysushruta0% (1)
- Article Wjpps 1530609494Document7 pagesArticle Wjpps 1530609494Vijaya DwarampudiNo ratings yet
- Sumathi ShatakamDocument22 pagesSumathi ShatakamVijaya DwarampudiNo ratings yet
- BD - Chaurasia's - Human - Anatomy, Volume 1 - Upper Limb Thorax, 6th Edition PDFDocument312 pagesBD - Chaurasia's - Human - Anatomy, Volume 1 - Upper Limb Thorax, 6th Edition PDFfiatbrava155183% (24)
- DM Dan Genetik, Who PDFDocument15 pagesDM Dan Genetik, Who PDFTri YuliasihNo ratings yet
- Need To Review Madhumeha Chikitsa According To Ayurvedic Pathophysiology For The Optimum Benefit of The PatientDocument17 pagesNeed To Review Madhumeha Chikitsa According To Ayurvedic Pathophysiology For The Optimum Benefit of The PatientVijaya DwarampudiNo ratings yet
- Literature Review: Surgical Management of Duodenal InjuryDocument34 pagesLiterature Review: Surgical Management of Duodenal InjuryTsega WesenNo ratings yet
- Superior MediastinumDocument4 pagesSuperior MediastinumYheng GaosaiiNo ratings yet
- The Respiratory Diaphragm in Osteopathic Vision - A Literature ReviewDocument6 pagesThe Respiratory Diaphragm in Osteopathic Vision - A Literature ReviewMarcus Dos SantosNo ratings yet
- Liver Function and AnatomyDocument2 pagesLiver Function and AnatomyKeanna Nicole CollantesNo ratings yet
- 2 Female Pelvis and Foetal SkullDocument17 pages2 Female Pelvis and Foetal SkullMalak Ahmed 2295No ratings yet
- General Arrangement of The Abdominal VisceraDocument30 pagesGeneral Arrangement of The Abdominal Visceraapi-249972919100% (2)
- Embro MCQ 2015Document15 pagesEmbro MCQ 2015Tofik MohammedNo ratings yet
- Anatomy of OesophagusDocument24 pagesAnatomy of OesophagusLia Restimulia DelfitriNo ratings yet
- Material Mini NetterDocument13 pagesMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNo ratings yet
- Minimally Invasive Surgery in Gynecological Practice: Ertan Sarıdoğan, Gokhan Sami Kilic, Kubilay Ertan (Ed.)Document332 pagesMinimally Invasive Surgery in Gynecological Practice: Ertan Sarıdoğan, Gokhan Sami Kilic, Kubilay Ertan (Ed.)salah subbahNo ratings yet
- Abdomen: Radiology RevisionDocument11 pagesAbdomen: Radiology RevisionhimaniNo ratings yet
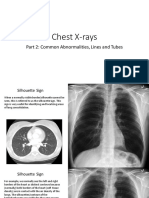
- Chest Xray PT 2Document41 pagesChest Xray PT 2pvs5155No ratings yet
- Rectum Anal CanalDocument24 pagesRectum Anal CanalsrijitNo ratings yet
- Surgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiDocument10 pagesSurgical Techniques For Pancreas Transplantation: Ugo Boggi, Gabriella Amorese and Piero MarchettiNatalindah Jokiem Woecandra T. D.No ratings yet
- Urinary System - Gross 2016Document73 pagesUrinary System - Gross 2016dawnparkNo ratings yet
- Radiation Oncology - Toxicity - RTOG - Wikibooks, Open Books For An Open WorldDocument15 pagesRadiation Oncology - Toxicity - RTOG - Wikibooks, Open Books For An Open WorldJosep GamarraNo ratings yet
- Breathing Made Simple E-BookDocument17 pagesBreathing Made Simple E-BookErin100% (1)
- Anatomy of The Female Reproductive SystemDocument111 pagesAnatomy of The Female Reproductive SystemGetinetNo ratings yet
- Esophageal Reconstruction With Small IntestineDocument22 pagesEsophageal Reconstruction With Small IntestineCitra AryantiNo ratings yet
- Variations in Dimensions and Shape of ThoracicDocument10 pagesVariations in Dimensions and Shape of Thoracicerika_mak23No ratings yet
- Struktur Morfologi Dan Anatomi Burung Endemik Sulawesi Cabai Panggul-Kelabu (Dicaeum Celebicum Műller, 1843)Document7 pagesStruktur Morfologi Dan Anatomi Burung Endemik Sulawesi Cabai Panggul-Kelabu (Dicaeum Celebicum Műller, 1843)SaadatulNo ratings yet
- Paraplegia Due To Incomplete Spinal Cord Injury: Orthopedic and Traumatology Department Hasanuddin UniversityDocument56 pagesParaplegia Due To Incomplete Spinal Cord Injury: Orthopedic and Traumatology Department Hasanuddin UniversitySt. Nur SyamsiahNo ratings yet
- Gross Anatomy and Histolgy of UrinarysystemDocument81 pagesGross Anatomy and Histolgy of UrinarysystemIncredible DivineNo ratings yet
- Abdominal Exercises: A Review Study For Training PrescriptionDocument4 pagesAbdominal Exercises: A Review Study For Training PrescriptioninventionjournalsNo ratings yet
- Blood Supply of Head and NeckDocument29 pagesBlood Supply of Head and NeckBM mugalNo ratings yet
- Trauma Tulang Belakang-Ppgd - Dr. YoyosDocument57 pagesTrauma Tulang Belakang-Ppgd - Dr. YoyoszaroziNo ratings yet
- Abnormalities of The Passage-WilliamsDocument66 pagesAbnormalities of The Passage-Williamsapi-19641337100% (1)
- Step by Step Lihation of The Internal Iliac ArteryDocument6 pagesStep by Step Lihation of The Internal Iliac ArteryAkbar PurnadiputraNo ratings yet
- Anaphy Concept MappingDocument3 pagesAnaphy Concept MappingArlynn MartinezNo ratings yet
- Operative Anatomy of The HeartDocument559 pagesOperative Anatomy of The HeartHenrique MaiaNo ratings yet