You might also like
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- Jantung Sebagai PompaDocument54 pagesJantung Sebagai PompaIndraYudhiNo ratings yet
- Cvs PPT 2) BpehssDocument35 pagesCvs PPT 2) BpehssAmbreen GhafoorNo ratings yet
- Electrical Conduction in The HeartDocument35 pagesElectrical Conduction in The HeartNormasnizam Mohd NoorNo ratings yet
- Lecture-5 Cardiac CycleDocument28 pagesLecture-5 Cardiac Cyclettalhalatif99No ratings yet
- Cardiac Cycle by Bala GoyalDocument14 pagesCardiac Cycle by Bala Goyaltee su lingNo ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleAdel100% (1)
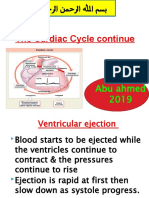
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- K - 12 Heart As A Pump (Fisiologi)Document36 pagesK - 12 Heart As A Pump (Fisiologi)missirenaNo ratings yet
- Oral PathologyDocument23 pagesOral PathologyRuba AbbassNo ratings yet
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- Cardiac Physiology PDFDocument17 pagesCardiac Physiology PDFAli Aborges Jr.No ratings yet
- 8.1b. Systole-Diastole & Cardiac CycleDocument34 pages8.1b. Systole-Diastole & Cardiac Cycleverysedatedx100% (1)
- Cardiac CycleDocument30 pagesCardiac CycleCarrine Liew100% (2)
- Cardiovascular PhysiologyDocument88 pagesCardiovascular Physiologykhorrami4No ratings yet
- Cardiac Cycle: DR Rakesh JainDocument97 pagesCardiac Cycle: DR Rakesh JainKemoy FrancisNo ratings yet
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 pagesThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanNo ratings yet
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 pagesThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanNo ratings yet
- Cv-4 PHDocument28 pagesCv-4 PHaya najemNo ratings yet
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDocument46 pagesCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Document6 pages04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsNo ratings yet
- CARDIAC CYCLE-laDocument12 pagesCARDIAC CYCLE-latehillahkabwe100No ratings yet
- Cardiac CycleDocument31 pagesCardiac CycleAdwaitha KrNo ratings yet
- 01 - Cardiac CycleDocument4 pages01 - Cardiac CycleEhtiram HuseynovNo ratings yet
- Cardiac CycleDocument18 pagesCardiac CycleKundan GuptaNo ratings yet
- PC Cardiac CycleDocument29 pagesPC Cardiac CycleSebontu HasenNo ratings yet
- 4,5-Cardiac Cycle Team441Document29 pages4,5-Cardiac Cycle Team441aliusman laseNo ratings yet
- Cardiovascular Physiology: October 25, 2010Document51 pagesCardiovascular Physiology: October 25, 2010VinuPrakashJ.No ratings yet
- Cardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyDocument27 pagesCardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyThird Year B PharmNo ratings yet
- CV Physio-IntroductionDocument33 pagesCV Physio-IntroductionHanaNo ratings yet
- Study FastDocument49 pagesStudy FastmbbsporalekhaNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- Cardiac Cycle: DR Rida Ajmal KhanDocument29 pagesCardiac Cycle: DR Rida Ajmal KhanMooma fatimaNo ratings yet
- Circulatory SystemDocument304 pagesCirculatory Systemyapyihao2100% (1)
- Intracardiac PressuresDocument41 pagesIntracardiac Pressureswaleed315No ratings yet
- Amboss - Cradiac CycleDocument18 pagesAmboss - Cradiac CycleAllysahNo ratings yet
- Cardiac Cycle - DR Rakesh JainDocument97 pagesCardiac Cycle - DR Rakesh JainEmmieNo ratings yet
- Physiology 09Document36 pagesPhysiology 09Sumeyya Binte BockthierNo ratings yet
- Cardiac CycleDocument5 pagesCardiac Cyclen_nkNo ratings yet
- CVS - IiDocument12 pagesCVS - IiBinta Elsa JohnNo ratings yet
- Heart Sounds and Arteriovenous Pulses: DR Chandana HewageDocument48 pagesHeart Sounds and Arteriovenous Pulses: DR Chandana HewagePrasad HewawasamNo ratings yet
- Cardiac Cycle: Himawan WDocument46 pagesCardiac Cycle: Himawan WaprinaNo ratings yet
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Physiology Shet #7&8Document12 pagesPhysiology Shet #7&8Rawan Abu HammourNo ratings yet
- DR Rahimah Zakaria Dept of PhysiologyDocument31 pagesDR Rahimah Zakaria Dept of PhysiologyChokJunHoongNo ratings yet
- K-12 Heart As A Pump - CVS-K12Document37 pagesK-12 Heart As A Pump - CVS-K12Jane Andrea Christiano DjianzonieNo ratings yet
- Cardiovascular SystemDocument6 pagesCardiovascular SystemJeminah Fae CalmaNo ratings yet
- Physiology of The Cardiac SystemDocument41 pagesPhysiology of The Cardiac SystemRoh JitenNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- 3 Cardiology HemodynamicsDocument90 pages3 Cardiology HemodynamicsPravallika ReddyNo ratings yet
- The Cardiac Cycle: Describing The Sequence of Events in One Heart BeatDocument14 pagesThe Cardiac Cycle: Describing The Sequence of Events in One Heart BeatAswathy KrishnaNo ratings yet
- Cardiovascular Physiology 3Document69 pagesCardiovascular Physiology 3maxmus4No ratings yet
- Chapter 020Document54 pagesChapter 020Mar3RDi MusicNo ratings yet
- 5 Cardiac Cycle & Heart SoundsDocument32 pages5 Cardiac Cycle & Heart SoundsDisha SuvarnaNo ratings yet
- DR Najeeb Cardiac CycleDocument5 pagesDR Najeeb Cardiac Cycleعلي. احمد100% (1)
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Document68 pagesKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraNo ratings yet
- The Cardiac Cycle NotesDocument5 pagesThe Cardiac Cycle NotesAsad Khan Khalil100% (1)
- Cardiac Cycle CardiodynamicsDocument29 pagesCardiac Cycle Cardiodynamicseverforyou2023No ratings yet
- Departemen Bedah Mulut Dan Maksilofasial FKG Usu: ISNANDAR, DRG., SP - BMDocument43 pagesDepartemen Bedah Mulut Dan Maksilofasial FKG Usu: ISNANDAR, DRG., SP - BMXeniel AlastairNo ratings yet
- DR - Nuraiza Meutia, M.Biomed: Dept - Fisiologi FK USU Prof. Yasmeiny YazirDocument49 pagesDR - Nuraiza Meutia, M.Biomed: Dept - Fisiologi FK USU Prof. Yasmeiny YazirXeniel AlastairNo ratings yet
- K31a - Electrophysiology and Cardiac Arrhytmia EmergencyDocument46 pagesK31a - Electrophysiology and Cardiac Arrhytmia EmergencyXeniel AlastairNo ratings yet
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairNo ratings yet
- (K29) Electrocardiogram CVSDocument43 pages(K29) Electrocardiogram CVSXeniel AlastairNo ratings yet
- (K7) Valvular Heart DiseaseDocument79 pages(K7) Valvular Heart DiseaseXeniel AlastairNo ratings yet
- Rheumatic Fever AND Rheumatic Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuDocument15 pagesRheumatic Fever AND Rheumatic Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuXeniel AlastairNo ratings yet
- Risk Preterm: "Nerves" and Depression, Help From Professional Agencies, and Little Contact of PretermDocument3 pagesRisk Preterm: "Nerves" and Depression, Help From Professional Agencies, and Little Contact of PretermXeniel AlastairNo ratings yet
- Female Reproductive System: Praktikum KBK Semester VDocument44 pagesFemale Reproductive System: Praktikum KBK Semester VXeniel AlastairNo ratings yet
- Anatomy and Physiology of The Cardiovascular System Medical Surgical NursingDocument68 pagesAnatomy and Physiology of The Cardiovascular System Medical Surgical NursingFelix NjakeNo ratings yet
- Cardio Book PDFDocument34 pagesCardio Book PDFDwi PascawitasariNo ratings yet
- Double CirculationDocument2 pagesDouble CirculationMonika KanojiaNo ratings yet
- Test Bank For Human Diseases 8th Edition ZelmanDocument22 pagesTest Bank For Human Diseases 8th Edition Zelmandenisedanielsbkgqyzmtr100% (29)
- Transport System in HumanDocument16 pagesTransport System in HumanHtet Htet NaingNo ratings yet
- Physiology of The Cardiovascular System-CVSDocument56 pagesPhysiology of The Cardiovascular System-CVSAmanuel MaruNo ratings yet
- Pre Eclampsia - FinalDocument54 pagesPre Eclampsia - Finalsupernurse02No ratings yet
- The Cardiovascular System: Elaine N. MariebDocument46 pagesThe Cardiovascular System: Elaine N. MariebIvann Chan MunarNo ratings yet
- The Cardiovascular SystemDocument13 pagesThe Cardiovascular SystemCaraDeleNo ratings yet
- 10.2 Circulatory System: Group 2Document15 pages10.2 Circulatory System: Group 2DANISTTA A/P LOGARAJAH MoeNo ratings yet
- Nursing Care During Normal Pregnancy Care of Dev FetusDocument5 pagesNursing Care During Normal Pregnancy Care of Dev FetusLuna Sang-anNo ratings yet
- Lab Manual Bio II 201701Document79 pagesLab Manual Bio II 201701Charlie LaiNo ratings yet
- Cardiac Ana & DxticsDocument3 pagesCardiac Ana & Dxticsjames garciaNo ratings yet
- Atlas of Critical Care EchocardiographyDocument189 pagesAtlas of Critical Care EchocardiographyAnna Anna100% (1)
- Grade 9Document2 pagesGrade 9letty lou0% (1)
- Neoreviews 1 2018Document69 pagesNeoreviews 1 2018Raul VillacresNo ratings yet
- Human Body - Heart and Circulatory System PDFDocument113 pagesHuman Body - Heart and Circulatory System PDFWalter Silva Serrano100% (5)
- Anatomy & Physiology of Farm Animals: By: Eddie C. Bautista Jr. DVM, MSADocument221 pagesAnatomy & Physiology of Farm Animals: By: Eddie C. Bautista Jr. DVM, MSAJayson BasiagNo ratings yet
- Dental Care For Patients With Heart Failure: An UpdateDocument9 pagesDental Care For Patients With Heart Failure: An UpdateGustavo A OrtegonNo ratings yet
- Tetralogy of FallotDocument3 pagesTetralogy of FallotJohn Mark PocsidioNo ratings yet
- مذكرة علوم للصف الخامس الابتدائي الترم الثاني لغات science for primary second term 2015Document37 pagesمذكرة علوم للصف الخامس الابتدائي الترم الثاني لغات science for primary second term 2015rabei87% (23)
- Nursing Manual OptDocument151 pagesNursing Manual OptNjoku StephenNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Anatomy of The HeartDocument28 pagesAnatomy of The HeartHerman DjawaNo ratings yet
- 6 Types of CirculationDocument14 pages6 Types of CirculationRolandoNo ratings yet
- Circ TESTDocument5 pagesCirc TESTCabo VlogNo ratings yet
- Chapter 42 Sample Questions and AnswersDocument3 pagesChapter 42 Sample Questions and AnswersLandry BrownNo ratings yet
- Bcse (SMR)Document182 pagesBcse (SMR)Muhammad Sajid100% (2)
- Science 9 q1 Mod1 Respiratory and Circulatory System Ver FinalDocument33 pagesScience 9 q1 Mod1 Respiratory and Circulatory System Ver Finalglam glitzNo ratings yet
- SS1 1ST Term Animal Husbandry E-NoteDocument29 pagesSS1 1ST Term Animal Husbandry E-Notekanajoseph2009No ratings yet