You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Lecture-35 Eectronic Fetal MonitoringDocument45 pagesLecture-35 Eectronic Fetal MonitoringMadhu Sudhan PandeyaNo ratings yet
- Lecture-33 Postpartum HemorrhageDocument50 pagesLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- POGS Practice Bulletin 3 FINALDocument6 pagesPOGS Practice Bulletin 3 FINALAileen TombocNo ratings yet
- Final Examination With Answers and RationalesDocument114 pagesFinal Examination With Answers and RationalesMonicaNo ratings yet
- Ectopic PregnancyDocument45 pagesEctopic PregnancyHoney May Rollan VicenteNo ratings yet
- Tubal Ectopic Pregnancy PB193Document13 pagesTubal Ectopic Pregnancy PB193Sheyla Orellana PurillaNo ratings yet
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaNo ratings yet
- Assignment On Obstetrics and Gynaecology DepartmentDocument14 pagesAssignment On Obstetrics and Gynaecology Departmentbhavnil_1796No ratings yet
- Kehamilan Ektopik TergangguDocument31 pagesKehamilan Ektopik TergangguAnonymous al0G68RwjJNo ratings yet
- Introduction About SelfDocument27 pagesIntroduction About SelfsimonjosanNo ratings yet
- श्रम एेन २०७४Document53 pagesश्रम एेन २०७४PradIpta Kaphle0% (1)
- Quick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountDocument2 pagesQuick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountMadhu Sudhan Pandeya100% (1)
- Who Rights Roles Respon HW Covid 19Document3 pagesWho Rights Roles Respon HW Covid 19HarryNo ratings yet
- Nepal Medical Council Act, 2020 (1964)Document20 pagesNepal Medical Council Act, 2020 (1964)Madhu Sudhan PandeyaNo ratings yet
- Abortion: Renhe Hospital Wang JunjieDocument51 pagesAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaNo ratings yet
- Voter ListDocument214 pagesVoter ListMadhu Sudhan PandeyaNo ratings yet
- Lecture-11 Breech PresentationDocument27 pagesLecture-11 Breech PresentationMadhu Sudhan PandeyaNo ratings yet
- Lecture-26 Hypertensive Disease of PregnancyDocument28 pagesLecture-26 Hypertensive Disease of PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaNo ratings yet
- Vaccination Guideline: International Travel and Health 2007Document9 pagesVaccination Guideline: International Travel and Health 2007Madhu Sudhan PandeyaNo ratings yet
- Teratology & Chronic PoisoningDocument54 pagesTeratology & Chronic PoisoningMadhu Sudhan PandeyaNo ratings yet
- Lecture-17 Shoulder DystociaDocument20 pagesLecture-17 Shoulder DystociaMadhu Sudhan PandeyaNo ratings yet
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDocument98 pagesPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan PandeyaNo ratings yet
- Lecture-22 Prolonged PregnancyDocument24 pagesLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaNo ratings yet
- Lecture-25 Cesarean SectionDocument21 pagesLecture-25 Cesarean SectionMadhu Sudhan PandeyaNo ratings yet
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaNo ratings yet
- Bishop's Pre-Induction Cervical Scoring SystemDocument2 pagesBishop's Pre-Induction Cervical Scoring SystemMadhu Sudhan PandeyaNo ratings yet
- Lecture 30 PromDocument7 pagesLecture 30 PromMadhu Sudhan PandeyaNo ratings yet
- Lecture-13 Transeverse LieDocument15 pagesLecture-13 Transeverse LieMadhu Sudhan PandeyaNo ratings yet
- Lecture-15 Prolonged LaborDocument8 pagesLecture-15 Prolonged LaborMadhu Sudhan PandeyaNo ratings yet
- Lecture-6 Obstetric TerminologiesDocument17 pagesLecture-6 Obstetric TerminologiesMadhu Sudhan PandeyaNo ratings yet
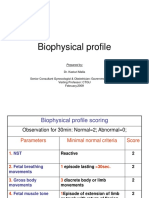
- Lecture-23 Biophysical ProfieDocument3 pagesLecture-23 Biophysical ProfieMadhu Sudhan PandeyaNo ratings yet
- Lecture-12 Face PresentationDocument9 pagesLecture-12 Face PresentationMadhu Sudhan PandeyaNo ratings yet
- Cord ProlapseDocument7 pagesCord ProlapseMadhu Sudhan PandeyaNo ratings yet
- Lecture-24 Twins PregnancyDocument30 pagesLecture-24 Twins PregnancyMadhu Sudhan PandeyaNo ratings yet
- Surgicopath June, 2018 FinalDocument115 pagesSurgicopath June, 2018 FinalPencenk AzznewNo ratings yet
- SALphingoDocument3 pagesSALphingoGhileen AbalosNo ratings yet
- Ectopic PregnancyDocument39 pagesEctopic PregnancyFecky Fihayatul IchsanNo ratings yet
- Ectopic Pregnancy Treatment & ManagementDocument12 pagesEctopic Pregnancy Treatment & ManagementDebi SumarliNo ratings yet
- Codorniz-Module 5 - DeontologyDocument3 pagesCodorniz-Module 5 - DeontologyJoshua CodornizNo ratings yet
- EctopicDocument13 pagesEctopicAnonymous P5efHbeNo ratings yet
- KKPMT IV B ICD 9 Female GenitaliaDocument31 pagesKKPMT IV B ICD 9 Female GenitaliaAldy SetyawanNo ratings yet
- Tubal Ligation and Salpingectomy and The Risk of Epithelial Ovarian CancerDocument6 pagesTubal Ligation and Salpingectomy and The Risk of Epithelial Ovarian CancerAlyssa MarzanNo ratings yet
- Dr. Sourav Chowdhury Senior ResidentDocument79 pagesDr. Sourav Chowdhury Senior ResidentBhawna JoshiNo ratings yet
- Diagnostic Clues To Ectopic PregnancyDocument3 pagesDiagnostic Clues To Ectopic Pregnancydrajayhalder9192No ratings yet
- CREOGGYNREVIEW PP PDFDocument98 pagesCREOGGYNREVIEW PP PDFRima HajjarNo ratings yet
- Ectopic Pregnancy - PowerpointDocument60 pagesEctopic Pregnancy - PowerpointAndrada Doţa100% (1)
- Wesleyan University - Philippines: Surgical Scrub Cases (Major)Document5 pagesWesleyan University - Philippines: Surgical Scrub Cases (Major)Kristine CastilloNo ratings yet
- Ectopic PregnancyDocument39 pagesEctopic PregnancyMuhammad SherazNo ratings yet
- Embarazo Ectopico Tubarico ACOG 2018Document13 pagesEmbarazo Ectopico Tubarico ACOG 2018Jesus SuarezNo ratings yet
- Icd 9 Obstetri N Gynek Plus TindakanDocument4 pagesIcd 9 Obstetri N Gynek Plus TindakanMimi Nanda Miranda AnastasiaNo ratings yet
- Ectopic Pregnancy FocusDocument62 pagesEctopic Pregnancy FocusrajaeasNo ratings yet
- Sistem Reproduksi Wanita-Uswatun Hasanah 195037Document13 pagesSistem Reproduksi Wanita-Uswatun Hasanah 195037Uswatun HasanahNo ratings yet
- Prosedur Tindakan Yang Sering Dilakukan Sesuai ICD9CMDocument8 pagesProsedur Tindakan Yang Sering Dilakukan Sesuai ICD9CMnovi rista anandaNo ratings yet
- Williams Gynecology Fourth Edition Joseph I Schaffer Barbara L Hoffman Karen D Bradshaw Lisa M Halvorson Marlene M Corton John O Schorge All ChapterDocument68 pagesWilliams Gynecology Fourth Edition Joseph I Schaffer Barbara L Hoffman Karen D Bradshaw Lisa M Halvorson Marlene M Corton John O Schorge All Chaptervicky.shelby900100% (16)
- Ectopic PregnancyDocument7 pagesEctopic PregnancyDeepshikha MahapatraNo ratings yet
- (OB2) Quiz 1 - Bleeding in 1st Half of Pregnancy (2020)Document5 pages(OB2) Quiz 1 - Bleeding in 1st Half of Pregnancy (2020)Jolaine ValloNo ratings yet
- Ectopic Pregnancy TR&JCDocument55 pagesEctopic Pregnancy TR&JCMeaw Thitirat SupasilNo ratings yet