You might also like
- Ortopedic TestsDocument4 pagesOrtopedic TestsdocfinNo ratings yet
- Special TestsDocument12 pagesSpecial Testspfi_jenNo ratings yet
- Anatomy Moore FlashcardsDocument6 pagesAnatomy Moore FlashcardsWade BullockNo ratings yet
- Week 2 Ortho Tests Figure NoDocument14 pagesWeek 2 Ortho Tests Figure Noapi-468597987No ratings yet
- Shoulder Exam: Inspection, Palpation, ROM, Special TestsDocument8 pagesShoulder Exam: Inspection, Palpation, ROM, Special Testsbrokenlimit5No ratings yet
- Specialtest Knee 140720123835 Phpapp01 PDFDocument146 pagesSpecialtest Knee 140720123835 Phpapp01 PDFlaszlo-368875100% (1)
- Joint Exam Special Test ReviewDocument4 pagesJoint Exam Special Test ReviewNish ShahNo ratings yet
- Eaxminarea ArticularaDocument40 pagesEaxminarea Articularaadelinamihaela7No ratings yet
- Workshop PPT (Final) Knee JointDocument127 pagesWorkshop PPT (Final) Knee Jointpasha100% (2)
- Week 6 - PCPDocument6 pagesWeek 6 - PCPapi-479754549No ratings yet
- Special Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With ADocument32 pagesSpecial Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With AnatkwqNo ratings yet
- Skeletal Muscle System OSCE ExaminationDocument14 pagesSkeletal Muscle System OSCE ExaminationMaryam A Albalooshi100% (2)
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- Week 4 Ortho TestsDocument15 pagesWeek 4 Ortho Testsapi-468597987No ratings yet
- Physical Examination of The Shoulder FinalDocument28 pagesPhysical Examination of The Shoulder FinalAndinNo ratings yet
- Compartment Syndrome Hand and ForearmDocument33 pagesCompartment Syndrome Hand and ForearmProfesseur Christian Dumontier100% (2)
- Orthopedic Shoulder ExaminationDocument4 pagesOrthopedic Shoulder Examinationapi-281340024No ratings yet
- Clinical Examination of Acute Adductor InjuriesDocument18 pagesClinical Examination of Acute Adductor Injuriessofianos100% (1)
- Shoulder Exam ChecklistDocument2 pagesShoulder Exam ChecklistJaymin BhattNo ratings yet
- Speed's test, biceps test, supraspinatus testsDocument8 pagesSpeed's test, biceps test, supraspinatus testsASM MutahirNo ratings yet
- Achilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAchilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Office Orthopaedics: Ramirez, Bryan Paul GDocument57 pagesOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezNo ratings yet
- Examination of The HandDocument20 pagesExamination of The HandOtnil DNo ratings yet
- Protocols MSK MRI (2010)Document123 pagesProtocols MSK MRI (2010)Danish218100% (1)
- Passive Scapular Adduction TestDocument15 pagesPassive Scapular Adduction Testapi-468597987No ratings yet
- Hip Examination - OSCE Guide - Geeky MedicsDocument6 pagesHip Examination - OSCE Guide - Geeky MedicsAmcDelhiNo ratings yet
- Patofisiology Urinary IncontinenceDocument45 pagesPatofisiology Urinary Incontinencesingle_ladyNo ratings yet
- Patofisiology Urinary IncontinenceDocument45 pagesPatofisiology Urinary Incontinencesingle_ladyNo ratings yet
- TM Shoulder Exam-1Document36 pagesTM Shoulder Exam-1ratkhiaberNo ratings yet
- ShoulderDocument51 pagesShoulderIts LaraNo ratings yet
- Sports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio BouffardDocument133 pagesSports Medicine and Musculoskeletal Ultrasound: A Pocket Guide Mouhanad M. El-Othmani Henry T. Goitz J. Antonio Bouffardnzkvw6s92hNo ratings yet
- Elbow TestsDocument30 pagesElbow TestsSuleiman AbdallahNo ratings yet
- Exercise & Nutrition for Managing OsteoporosisDocument73 pagesExercise & Nutrition for Managing Osteoporosissingle_ladyNo ratings yet
- Anatomy Concept Book AtfDocument246 pagesAnatomy Concept Book AtfRishi ShekharNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Pemeriksann Fisis Tulang BelakangDocument78 pagesPemeriksann Fisis Tulang BelakangulfianiNo ratings yet
- Elbow AssessmentDocument39 pagesElbow AssessmentshizarahimNo ratings yet
- Orthopaedic Special TestDocument24 pagesOrthopaedic Special TestpradhanaadhityaNo ratings yet
- Reading Knee - RamaDocument33 pagesReading Knee - RamavjhvghcghcghghNo ratings yet
- Dannys Special TestsDocument17 pagesDannys Special Testsapi-323342594No ratings yet
- Physical Ex of ElbowDocument23 pagesPhysical Ex of ElbowNgurah AndhikaNo ratings yet
- Shoulder InstabilityDocument57 pagesShoulder Instabilityashithoshn06No ratings yet
- Pemeriksaan Fisik LututDocument54 pagesPemeriksaan Fisik LututShone NamNo ratings yet
- Spine Exam 2Document44 pagesSpine Exam 2Azmi FarhadiNo ratings yet
- Cervical RibDocument15 pagesCervical RibArko duttaNo ratings yet
- Physioterapy SalveDocument45 pagesPhysioterapy SalveIkhar KeliobasNo ratings yet
- WK 4 Study QsDocument4 pagesWK 4 Study Qsapi-479720222No ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Elbow PT AssessmentDocument31 pagesElbow PT Assessmentkrissh20No ratings yet
- Ankylosing Spondylitis 1Document31 pagesAnkylosing Spondylitis 1Salman KhanNo ratings yet
- Forearm-Wrist-And-Hand-Ortho TestsDocument21 pagesForearm-Wrist-And-Hand-Ortho TestsMohammad Amjad KhanNo ratings yet
- SHOULDER EXAM GUIDEDocument8 pagesSHOULDER EXAM GUIDEZia Ur RehmanNo ratings yet
- Upper Extremity Special Tests GuideDocument7 pagesUpper Extremity Special Tests GuideRiaz KhanNo ratings yet
- Musculoskeletal System Name-Purushothaman Sabarigiri 1 Year Sec - IDocument31 pagesMusculoskeletal System Name-Purushothaman Sabarigiri 1 Year Sec - INuhu BankwhotNo ratings yet
- Ortho VertDocument4 pagesOrtho VertfelixhartantoNo ratings yet
- Special Tests For Cervical RadiculopathyDocument19 pagesSpecial Tests For Cervical RadiculopathyNamrata SharmaNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- PE and Diagnosis of ElbowDocument58 pagesPE and Diagnosis of Elbowmupt77No ratings yet
- Activity AssesmentDocument4 pagesActivity AssesmentGuillana Mae CastellonNo ratings yet
- Pe FixDocument38 pagesPe FixNgurah AndhikaNo ratings yet
- WK 3 Chiro TableDocument4 pagesWK 3 Chiro Tableapi-469904011No ratings yet
- Elbow TestsDocument12 pagesElbow TestsAqsa ZaheerNo ratings yet
- Hawkins-Kennedy Test: Humerus LigamentDocument7 pagesHawkins-Kennedy Test: Humerus LigamentlewienNo ratings yet
- Special TestsDocument124 pagesSpecial TestsMaitryChhedaNo ratings yet
- Range of Motion Techniques for Cervical, Lumbar, Hip, Knee, Ankle and HandDocument22 pagesRange of Motion Techniques for Cervical, Lumbar, Hip, Knee, Ankle and HandnoureenNo ratings yet
- ultt26-03-2020-231022061259-7f0a393fDocument24 pagesultt26-03-2020-231022061259-7f0a393fSri Ram 07No ratings yet
- Shoulder Tests GuideDocument6 pagesShoulder Tests Guidedina sharafNo ratings yet
- Upper & Lower Limb ExaminationDocument20 pagesUpper & Lower Limb Examinationcvmqx7yppd100% (1)
- Patfis Valvular Heart DiseaseDocument1 pagePatfis Valvular Heart Diseasesingle_ladyNo ratings yet
- Patfis Valvular Heart DiseaseDocument1 pagePatfis Valvular Heart Diseasesingle_ladyNo ratings yet
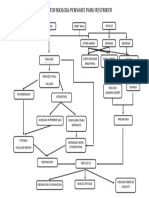
- Paru RestriktifDocument1 pageParu Restriktifsingle_ladyNo ratings yet
- Dasar VentilatorDocument40 pagesDasar Ventilatorsingle_ladyNo ratings yet
- Collaborative Practice With Nurses in Incontinence CareDocument25 pagesCollaborative Practice With Nurses in Incontinence Caresingle_ladyNo ratings yet
- Kinesiology ElbowDocument53 pagesKinesiology Elbowsingle_ladyNo ratings yet
- Tatalaksana Rehabilitasi Penyakit Jantung BawaanDocument38 pagesTatalaksana Rehabilitasi Penyakit Jantung Bawaansingle_ladyNo ratings yet
- Theraex For IKFRDocument130 pagesTheraex For IKFRsingle_ladyNo ratings yet
- Tatalaksana Rehabilitasi Penyakit Jantung BawaanDocument38 pagesTatalaksana Rehabilitasi Penyakit Jantung Bawaansingle_ladyNo ratings yet
- Management of Acute Achilles Tendon RuptureDocument226 pagesManagement of Acute Achilles Tendon RuptureAnjatNo ratings yet
- Pretest Kardiorespi UnaDocument60 pagesPretest Kardiorespi Unasingle_ladyNo ratings yet
- Pathophysiology-Pathomechanics Dan Penegakan Diagnosis OsteoporosisDocument90 pagesPathophysiology-Pathomechanics Dan Penegakan Diagnosis Osteoporosissingle_ladyNo ratings yet
- Case Pediatri Cerebral PalsyDocument20 pagesCase Pediatri Cerebral Palsysingle_ladyNo ratings yet
- Pathophysiology-Pathomechanics Dan Penegakan Diagnosis OsteoporosisDocument90 pagesPathophysiology-Pathomechanics Dan Penegakan Diagnosis Osteoporosissingle_ladyNo ratings yet
- Physical Examination of The Knee: Oleh: Dr. Darsuna Mardhiah Pembimbing: Dr. Deta Tanuwidjaja, SP - KFRDocument36 pagesPhysical Examination of The Knee: Oleh: Dr. Darsuna Mardhiah Pembimbing: Dr. Deta Tanuwidjaja, SP - KFRsingle_ladyNo ratings yet
- Physical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,SpkfrDocument25 pagesPhysical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,Spkfrsingle_ladyNo ratings yet
- Disorders of The Knee FebyDocument19 pagesDisorders of The Knee Febysingle_ladyNo ratings yet
- Disorders of The Knee FebyDocument19 pagesDisorders of The Knee Febysingle_ladyNo ratings yet
- Case Report IdentityDocument16 pagesCase Report Identitysingle_ladyNo ratings yet
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyNo ratings yet
- Elbow AbnormalDocument21 pagesElbow Abnormalsingle_ladyNo ratings yet
- Physical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,SpkfrDocument25 pagesPhysical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,Spkfrsingle_ladyNo ratings yet
- Common Problem of HIPDocument40 pagesCommon Problem of HIPsingle_ladyNo ratings yet
- Splinting: Darsuna Mardhiah Dr. Tertianto Prabowo, SP - KFRDocument79 pagesSplinting: Darsuna Mardhiah Dr. Tertianto Prabowo, SP - KFRsingle_ladyNo ratings yet
- Short Case II: Jufri Febrianto, MDDocument16 pagesShort Case II: Jufri Febrianto, MDsingle_ladyNo ratings yet
- Muscles of The BackDocument2 pagesMuscles of The BackavrilaNo ratings yet
- Forearm, Hand and Wrist AnatomyDocument29 pagesForearm, Hand and Wrist AnatomyLeonard EllerbeNo ratings yet
- Pectoralis Biceps Obliques Rectus Abdominus Deltoid QuadricepsDocument2 pagesPectoralis Biceps Obliques Rectus Abdominus Deltoid QuadricepsAni BayindiryanNo ratings yet
- Anatomy HWDocument4 pagesAnatomy HWTassnime SebaeiNo ratings yet
- Atlas of Human Anatomy - Including Student Consult Interactive Ancillaries and Guides1Document1 pageAtlas of Human Anatomy - Including Student Consult Interactive Ancillaries and Guides1JackTroviNo ratings yet
- The Scapula - Surfaces - Fractures - Winging - TeachMeAnatomyDocument3 pagesThe Scapula - Surfaces - Fractures - Winging - TeachMeAnatomymohit kumarNo ratings yet
- Qbank FormatDocument5 pagesQbank FormatpashaNo ratings yet
- Shoulder - LectureDocument82 pagesShoulder - LectureElizabethNo ratings yet
- Breast Anatomy Regions and Lymph Node DrainageDocument8 pagesBreast Anatomy Regions and Lymph Node DrainagedrhendyjuniorNo ratings yet
- Dermatomes of The Upper LimbDocument55 pagesDermatomes of The Upper LimbGideon WillieNo ratings yet
- MLPP & MCPDocument1 pageMLPP & MCPSawada TsunayoshiNo ratings yet
- Cools 2008 Screening The Athletes Shoulder ForDocument9 pagesCools 2008 Screening The Athletes Shoulder ForLucyFloresNo ratings yet
- Riche-Cannieu Anastomosis With Partial Transection of The Median NerveDocument3 pagesRiche-Cannieu Anastomosis With Partial Transection of The Median NerveAdam L. SchreiberNo ratings yet
- PRINCIPLES OF TENDON TRANSFERS EXPLAINEDDocument17 pagesPRINCIPLES OF TENDON TRANSFERS EXPLAINEDGirijashankar KhuntiaNo ratings yet
- Shoulder and Lower Limb Muscle TestsDocument1 pageShoulder and Lower Limb Muscle TestsDadaboo UaNo ratings yet
- Brachial Plexus: Dr. Sama-ul-Haque Dr. Nivin SharafDocument44 pagesBrachial Plexus: Dr. Sama-ul-Haque Dr. Nivin SharaffitrizeliaNo ratings yet
- Anatomy Job Interview Preparation GuideDocument8 pagesAnatomy Job Interview Preparation GuideVanitha DassariNo ratings yet
- Froz Rotator Cuff TendinitisDocument11 pagesFroz Rotator Cuff TendinitisestherNo ratings yet
- Physio Med Infographic ElbowDocument3 pagesPhysio Med Infographic ElbowLoredana TirsNo ratings yet
- Overview of The Anatomy of The Upper and Lower LimbsDocument59 pagesOverview of The Anatomy of The Upper and Lower LimbsCher TangNo ratings yet
- 293-Article Text-765-1-10-20210528Document8 pages293-Article Text-765-1-10-20210528Nurlaili AmaliaNo ratings yet
- Anatomy Workbook - Intrinsic Hand MusclesDocument7 pagesAnatomy Workbook - Intrinsic Hand MusclesMukt PatelNo ratings yet
- Cuestionario Kamath y StothardDocument4 pagesCuestionario Kamath y StothardPasha Camacho100% (1)
- Treating Scapular Dyskinesis Through RehabilitationDocument8 pagesTreating Scapular Dyskinesis Through RehabilitationYa ChenNo ratings yet