You might also like
- Anti Inflammatory DrugsDocument82 pagesAnti Inflammatory DrugsShardendu MishraNo ratings yet
- Anti-Inflammatory Drugs Class Notes 2023Document82 pagesAnti-Inflammatory Drugs Class Notes 2023Jacob MasikaNo ratings yet
- Anti-Inflammatory Drugs OPB AY1415Document40 pagesAnti-Inflammatory Drugs OPB AY1415Mohammad Hazamyn Hazrul HamzahNo ratings yet
- Clinical Toxicology: Dep. of Biopharmaceutics and Clinical PharmacyDocument32 pagesClinical Toxicology: Dep. of Biopharmaceutics and Clinical Pharmacymalak amerNo ratings yet
- NSAIDs: Mechanisms, Effects and UsesDocument43 pagesNSAIDs: Mechanisms, Effects and UsesRitu ShewaniNo ratings yet
- NSAIDSDocument19 pagesNSAIDSDonna Kelly DuranNo ratings yet
- NSAIDsDocument45 pagesNSAIDsAnamta AshfaqNo ratings yet
- Musculoskeletal DrugsDocument29 pagesMusculoskeletal DrugsjanulNo ratings yet
- Cytoprotective Agents: Presented By: Guided byDocument53 pagesCytoprotective Agents: Presented By: Guided bydrfatimarizNo ratings yet
- NSAIDs: Mechanisms, Uses and Adverse EffectsDocument43 pagesNSAIDs: Mechanisms, Uses and Adverse EffectsTes B FourieNo ratings yet
- UntitledDocument45 pagesUntitledTani BirlaNo ratings yet
- NSAIDSDocument38 pagesNSAIDSShahmir KhanNo ratings yet
- NSAIDs and analgesics used to treat pain and inflammationDocument23 pagesNSAIDs and analgesics used to treat pain and inflammationAliza maryNo ratings yet
- Classification A) Analgesics and Anti-InflammatoryDocument6 pagesClassification A) Analgesics and Anti-InflammatoryPROF DR SHAHMURAD100% (2)
- NSAIDs, DMARDs & Antigout1Document69 pagesNSAIDs, DMARDs & Antigout1Melissa SalayogNo ratings yet
- Steroidal Anti - Inflammatory Drugs: NsaidsDocument96 pagesSteroidal Anti - Inflammatory Drugs: NsaidsDR AbidNo ratings yet
- Final CPD PAIN MANAGEMENT LECTURE Edit 2Document57 pagesFinal CPD PAIN MANAGEMENT LECTURE Edit 2auliaNo ratings yet
- Pharmacology of Anti-Inflammatory Drugs: Corticosteroids and NSAIDsDocument3 pagesPharmacology of Anti-Inflammatory Drugs: Corticosteroids and NSAIDsMirza HassanNo ratings yet
- Non Steroidal Anti Inflammatory Drugs: NsaidsDocument58 pagesNon Steroidal Anti Inflammatory Drugs: NsaidsmahamoudNo ratings yet
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDocument65 pagesNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNo ratings yet
- Analgesics: Non-Steroidal Anti-Inflammatory Drugs andDocument8 pagesAnalgesics: Non-Steroidal Anti-Inflammatory Drugs andWilliam C ChishaNo ratings yet
- Antpyretic-Analgesic and Antinlammatory DrugsDocument38 pagesAntpyretic-Analgesic and Antinlammatory DrugskasondaNo ratings yet
- Analgesics Non OpioidDocument6 pagesAnalgesics Non Opioidhlouis8No ratings yet
- 8 Nsaids 08 08 2023Document31 pages8 Nsaids 08 08 2023ashwin kNo ratings yet
- Anti Pyretic 2013Document15 pagesAnti Pyretic 2013Faizah Al GhamdiNo ratings yet
- Indomethacin 392Document17 pagesIndomethacin 392Mahadie Hasan JahadNo ratings yet
- Anti Inflamatory Drugs AINSDocument39 pagesAnti Inflamatory Drugs AINSEl FaroukNo ratings yet
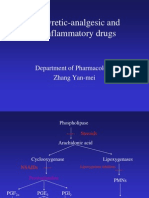
- Antipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiDocument39 pagesAntipyretic-Analgesic and Antiinflammatory Drugs: Department of Pharmacology Zhang Yan-MeiIshu SethiNo ratings yet
- Guide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsDocument40 pagesGuide to NSAIDs (Non-Steroidal Anti-Inflammatory DrugsHarini Bala100% (1)
- Modul Muskuloskeletal - NSAIDs 2017Document56 pagesModul Muskuloskeletal - NSAIDs 2017khairunnisanurainiNo ratings yet
- Analgesics - New Microsoft Office Power Point PresentationDocument21 pagesAnalgesics - New Microsoft Office Power Point Presentationrozha100% (4)
- NSAIDsDocument54 pagesNSAIDsAlaaNo ratings yet
- NsaidsDocument16 pagesNsaidsraffia mahakNo ratings yet
- B-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Document6 pagesB-Selective: I Group: Nonsteroidal Anti-Inflammatory Drugs (Nonsteroidal Ntiinflammatory)Moataz TrabehNo ratings yet
- NSAID Mechanism COX InhibitionDocument23 pagesNSAID Mechanism COX InhibitionWissam DadiNo ratings yet
- NsaidDocument29 pagesNsaidAnonymous vMjb3lQOPoNo ratings yet
- Anti Inflamasi Dan ANALGETIK (Anti Nociceptive)Document30 pagesAnti Inflamasi Dan ANALGETIK (Anti Nociceptive)SEPTIANA SAPUTRINo ratings yet
- NSAIDS PPT For MBBSDocument45 pagesNSAIDS PPT For MBBSVino ManiNo ratings yet
- Nsaid PDFDocument38 pagesNsaid PDFسامر الرفاعيNo ratings yet
- Nsaids: On Teroidal Nti Nflammatory RugDocument61 pagesNsaids: On Teroidal Nti Nflammatory RugNdayishimiye ErnestNo ratings yet
- 2020 Drugs On Pain (Analgesics) - DENTISTRYDocument28 pages2020 Drugs On Pain (Analgesics) - DENTISTRYVisayan Alliah GailNo ratings yet
- Anti-Inflammatory DrugsDocument36 pagesAnti-Inflammatory Drugsnezifzenu2023No ratings yet
- NsaidDocument17 pagesNsaidFirst LastNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs: Stephanie MonksDocument17 pagesNon-Steroidal Anti-Inflammatory Drugs: Stephanie MonkssteffmoNo ratings yet
- NSAIDsDocument12 pagesNSAIDsjelly100% (1)
- NSAIDs, DMARDs, Analgesics & Gout DrugsDocument114 pagesNSAIDs, DMARDs, Analgesics & Gout DrugsMani Jee100% (1)
- Saba Hanif Presentation...Document19 pagesSaba Hanif Presentation...Saba KhanNo ratings yet
- Pharm Chapter's Focus Review 2Document16 pagesPharm Chapter's Focus Review 2Briana SmetNo ratings yet
- Anti Inflammatory DrugsDocument40 pagesAnti Inflammatory DrugsTommy ZeusNo ratings yet
- NSAID Mechanism and UsesDocument11 pagesNSAID Mechanism and UsesSuranjan GhoshNo ratings yet
- NSAIDS 3, 4 SummaryDocument29 pagesNSAIDS 3, 4 SummaryAhmed ExaminationNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs (Nsaids) : DR ZareenDocument40 pagesNonsteroidal Anti-Inflammatory Drugs (Nsaids) : DR ZareenGareth BaleNo ratings yet
- NSAIDsDocument2 pagesNSAIDsRafiqul Haider LinkonNo ratings yet
- NSAIDDocument15 pagesNSAIDMaria KhawajaNo ratings yet
- Nonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharDocument97 pagesNonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharTarek NasrallahNo ratings yet
- NSAIDs: Non-steroidal Anti-inflammatory DrugsDocument45 pagesNSAIDs: Non-steroidal Anti-inflammatory DrugsArvi KhanNo ratings yet
- NSAIDsDocument2 pagesNSAIDsOm Prakash MishraNo ratings yet
- Lipid MediatorsFrom EverandLipid MediatorsFiona M. CunninghamNo ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
- Astellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeDocument3 pagesAstellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeHerry HendrayadiNo ratings yet
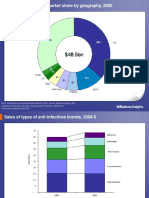
- The Global AntiInfectives Market OutlookDocument267 pagesThe Global AntiInfectives Market OutlookHerry HendrayadiNo ratings yet
- BCP 13010 PDFDocument11 pagesBCP 13010 PDFHerry HendrayadiNo ratings yet
- Practical Guide To Joint and Soft Tissue Injection TechniquesDocument5 pagesPractical Guide To Joint and Soft Tissue Injection TechniquesHerry HendrayadiNo ratings yet
- The Top 10 Generic Pharmaceutical CompaniesDocument10 pagesThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiNo ratings yet
- Standard Step-Wise Timelines in The Drug Discovery ProcessDocument19 pagesStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiNo ratings yet
- 1 - Dr. KungDocument18 pages1 - Dr. KungWawan IndrawanNo ratings yet
- Lifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingDocument176 pagesLifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingHerry Hendrayadi100% (1)
- Press Conference: Astellas' Growth StrategyDocument31 pagesPress Conference: Astellas' Growth StrategyHerry HendrayadiNo ratings yet
- The Top 10 Generic Pharmaceutical CompaniesDocument42 pagesThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiNo ratings yet
- The Top 10 Generic Pharmaceutical CompaniesDocument42 pagesThe Top 10 Generic Pharmaceutical CompaniesHerry HendrayadiNo ratings yet
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDocument176 pagesGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiNo ratings yet
- Achieving Market Dominance Through Reformulation.Document12 pagesAchieving Market Dominance Through Reformulation.Herry HendrayadiNo ratings yet
- The Global AntiInfectives Market OutlookDocument267 pagesThe Global AntiInfectives Market OutlookHerry HendrayadiNo ratings yet
- Top 10 Generic Pharmaceutical CompaniesDocument178 pagesTop 10 Generic Pharmaceutical CompaniesHerry HendrayadiNo ratings yet
- Indication Expansion Opportunities For Successful Lifecycle ManagementDocument144 pagesIndication Expansion Opportunities For Successful Lifecycle ManagementHerry HendrayadiNo ratings yet
- Standard Step-Wise Timelines in The Drug Discovery ProcessDocument19 pagesStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiNo ratings yet
- Global Market AnalysisaAntibioticsDocument23 pagesGlobal Market AnalysisaAntibioticsHerry HendrayadiNo ratings yet
- Pharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaDocument35 pagesPharmaceutical Growth Opportunities in Brazil, Russia, India and ChinaHerry HendrayadiNo ratings yet
- The Blockbuster Drugs Outlook PDFDocument259 pagesThe Blockbuster Drugs Outlook PDFHerry HendrayadiNo ratings yet
- Achieving Market Dominance Through ReformulationDocument223 pagesAchieving Market Dominance Through ReformulationHerry HendrayadiNo ratings yet
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsDocument176 pagesGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiNo ratings yet
- Pharma 2020 PWC ReportDocument32 pagesPharma 2020 PWC ReportBrand SynapseNo ratings yet
- Management Pocketbooks - The Balance Sheet PocketbookDocument309 pagesManagement Pocketbooks - The Balance Sheet PocketbookHerry Hendrayadi100% (1)
- Top 15 Therapeutic 2008 PDFDocument95 pagesTop 15 Therapeutic 2008 PDFHerry HendrayadiNo ratings yet
- 2nd Announcement A5 Upload 1Document18 pages2nd Announcement A5 Upload 1Herry HendrayadiNo ratings yet
- Ijss Aug Oa12Document5 pagesIjss Aug Oa12Herry HendrayadiNo ratings yet
- Reader's Digest January 2013Document148 pagesReader's Digest January 2013pereira_jus3430No ratings yet
- Systemic Lupus Erythematosus and Neuropsychiatric DiseaseDocument56 pagesSystemic Lupus Erythematosus and Neuropsychiatric DiseaseHerry HendrayadiNo ratings yet
- Pebc Sample QuestionDocument20 pagesPebc Sample QuestionSamiya Rinta100% (1)
- Bahan ReferatDocument17 pagesBahan ReferatGisma CNo ratings yet
- OB Case StudyDocument52 pagesOB Case StudyMaria ThereseNo ratings yet
- AUF SOM - Dse of Small Intestine PDFDocument166 pagesAUF SOM - Dse of Small Intestine PDFYestin Reece Corpus ArcegaNo ratings yet
- Ocp in Pcos PDFDocument38 pagesOcp in Pcos PDFKeeranmayeeishra0% (1)
- SleepDocument29 pagesSleepjosephnavyNo ratings yet
- Gym Beginners Common Questions AnsweredDocument2 pagesGym Beginners Common Questions AnsweredDr Abdullah SubhanNo ratings yet
- A MAN, GENRE APART: Dr. Avdhut BorkarDocument57 pagesA MAN, GENRE APART: Dr. Avdhut Borkarpediatric servicesNo ratings yet
- Esophageal Varices AMJDocument35 pagesEsophageal Varices AMJAli Al.JuffairiNo ratings yet
- Lucrare Stiintifica ParodontologieDocument4 pagesLucrare Stiintifica ParodontologieReduceriAvonNo ratings yet
- Central Acting Muscle Relaxants for Spasticity and SpasmsDocument12 pagesCentral Acting Muscle Relaxants for Spasticity and SpasmsKhemz Dalde LimNo ratings yet
- SALIVADocument68 pagesSALIVANimmi RenjithNo ratings yet
- Stridor, Aspiration, and Cough in ChildrenDocument41 pagesStridor, Aspiration, and Cough in ChildrenArif Rahman DmNo ratings yet
- Asymmetrical Hearing Loss: Jessica PrasadDocument6 pagesAsymmetrical Hearing Loss: Jessica PrasadSujaya ChattopadhyayNo ratings yet
- And&Dis&Ski&Cli&Atl&Jam&Els&Mcm&1 STDocument580 pagesAnd&Dis&Ski&Cli&Atl&Jam&Els&Mcm&1 STelliealderseyNo ratings yet
- Dr. Ronald Frans, SP - THT-KL, MKes.Document12 pagesDr. Ronald Frans, SP - THT-KL, MKes.alpriani patrasNo ratings yet
- Nursing Care Plan On: Ca OvaryDocument13 pagesNursing Care Plan On: Ca Ovaryvaishali TayadeNo ratings yet
- CHN Lec Finals UpdatedDocument69 pagesCHN Lec Finals UpdatedShainaChescaEvansNo ratings yet
- Antenatal Care Guideline Final of Final Submitted July 1st, 2021Document88 pagesAntenatal Care Guideline Final of Final Submitted July 1st, 2021Dina AmeNo ratings yet
- Case Study 2Document29 pagesCase Study 2drnasim20088171No ratings yet
- Responses To Metabolic Gi Liver Alterations Compiled HandoutsDocument185 pagesResponses To Metabolic Gi Liver Alterations Compiled HandoutsJoanna Taylan100% (1)
- 204 Questions On MicrobiologyDocument54 pages204 Questions On MicrobiologyMolly ThompsonNo ratings yet
- Balance-Retraining 7Document7 pagesBalance-Retraining 7Pilita Cases NardocciNo ratings yet
- SyringomyeliaDocument3 pagesSyringomyeliaAndi SanapatiNo ratings yet
- ADHD and The Americans With Disabilities ActDocument6 pagesADHD and The Americans With Disabilities Actdcowan100% (5)
- Cto 13 06 PDFDocument30 pagesCto 13 06 PDFDr.HarshNo ratings yet
- Bombay Blood GroupDocument1 pageBombay Blood GroupSanjay GuptaNo ratings yet
- 7@myelografiDocument39 pages7@myelografierly indrianiNo ratings yet
- Micro OBSDocument10 pagesMicro OBSMelchor Felipe SalvosaNo ratings yet