You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewDocument87 pages4 20190629 Detty Cochrane Indonesia UGM Champion Systematic ReviewRafaela LennyNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Picture, Flashcard, Worksheet: Date: September 16 2020 Grade: 1 Lesson: Parts of The FaceDocument2 pagesPicture, Flashcard, Worksheet: Date: September 16 2020 Grade: 1 Lesson: Parts of The FaceRafaela LennyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
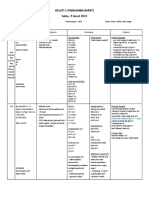
- Operan Jaga 5 Maret 2022Document29 pagesOperan Jaga 5 Maret 2022Rafaela LennyNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Sepsis. The Evolution in Definition, Pathophysiology, and ManagementDocument13 pagesSepsis. The Evolution in Definition, Pathophysiology, and ManagementIvan Tintaya UrureNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Edit Lenny - Functional Ileus - 23 Nov 19Document33 pagesEdit Lenny - Functional Ileus - 23 Nov 19Rafaela LennyNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Date: Grade: 3 Lesson: My HobbiesDocument2 pagesDate: Grade: 3 Lesson: My HobbiesRafaela LennyNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Example: A: "Would You Like To Count The Sum?" B: "OK" A: "Let's Count The Number" B: "OK"Document2 pagesExample: A: "Would You Like To Count The Sum?" B: "OK" A: "Let's Count The Number" B: "OK"Rafaela LennyNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Autoimmune Hemolytic Anemia During Pregnancy With Hemolytic Disease in The NewbornDocument6 pagesAutoimmune Hemolytic Anemia During Pregnancy With Hemolytic Disease in The NewbornRafaela LennyNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Assesmen Pasien GeriatriDocument7 pagesAssesmen Pasien GeriatriRafaela LennyNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Physics Holo - Lab Learning Experience: Using Smartglasses For Augmented Reality Labwork To Foster The Concepts of Heat ConductionDocument14 pagesPhysics Holo - Lab Learning Experience: Using Smartglasses For Augmented Reality Labwork To Foster The Concepts of Heat ConductionRafaela LennyNo ratings yet
- Functional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVDocument20 pagesFunctional Gastrointestinal Disorders History Pathophysiology Clinical Features and Rome IVwenyinriantoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- AUGMENTIN Syrup: What Is in This Leaflet?Document5 pagesAUGMENTIN Syrup: What Is in This Leaflet?Rafaela LennyNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Retinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Document7 pagesRetinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Rafaela LennyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Retinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Document7 pagesRetinopathy of Prematurity (ROP) : Melissa Andrews BME 281 Sec 2Rafaela LennyNo ratings yet
- TK03 Gagal Tumbuh Gabungan FinalDocument12 pagesTK03 Gagal Tumbuh Gabungan FinalRafaela LennyNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Impact of Duration of Using Superabsorbent Diaper On The Incidence of Urinary Tract Infection in Children 2161 0959.1000180Document5 pagesThe Impact of Duration of Using Superabsorbent Diaper On The Incidence of Urinary Tract Infection in Children 2161 0959.1000180Rafaela LennyNo ratings yet
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- 3399 On REG Congress CertificateDocument1 page3399 On REG Congress CertificateRafaela LennyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- DengueDocument67 pagesDengueRafaela LennyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- C.5 Encopresis 0072012Document14 pagesC.5 Encopresis 0072012Indah Afriani Nasution100% (1)
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- FIGOCEDocument11 pagesFIGOCEAldwin TanuwijayaNo ratings yet
- Functional Dyspepsia: Future Perspectives in GastroenterologyDocument77 pagesFunctional Dyspepsia: Future Perspectives in GastroenterologyRafaela LennyNo ratings yet
- Hunger Rating ScaleDocument1 pageHunger Rating ScaleRafaela LennyNo ratings yet
- Malaysia PRP Community Pharmacy LogbookDocument77 pagesMalaysia PRP Community Pharmacy LogbookAiWeiNo ratings yet
- NK GurbaniDocument24 pagesNK GurbanimedigistNo ratings yet
- WI Group Insurance Board Segal ReportDocument163 pagesWI Group Insurance Board Segal ReportMichelle FelberNo ratings yet
- Calcium Channel BlockersDocument35 pagesCalcium Channel BlockersSufyan MirzaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- J P S T: Studi Kepatuhan Pasien Diabetes Mellitus Rawat Jalan Di Rsud Kabupaten SidoarjoDocument10 pagesJ P S T: Studi Kepatuhan Pasien Diabetes Mellitus Rawat Jalan Di Rsud Kabupaten SidoarjoBerlianti Citra MaulidyaNo ratings yet
- Cultural and Spiritual Mnemonic Tools 11.06.09Document26 pagesCultural and Spiritual Mnemonic Tools 11.06.09Krisna May Buhisan PecoreNo ratings yet
- Communication Skill TrainingDocument6 pagesCommunication Skill TrainingjjpulikenNo ratings yet
- Landmark Recovery Petition and Stay With ExhibitsDocument92 pagesLandmark Recovery Petition and Stay With ExhibitsWNDUNo ratings yet
- Impact of Illness Lecture - HandoutDocument5 pagesImpact of Illness Lecture - HandoutRyan PanNo ratings yet
- Health Psychology A Textbook 7Th Edition Jane Ogden Full ChapterDocument67 pagesHealth Psychology A Textbook 7Th Edition Jane Ogden Full Chaptersteven.kincaid536100% (4)
- Effect of Whatsapp Reminder On Antenatal Care RevisitDocument11 pagesEffect of Whatsapp Reminder On Antenatal Care RevisitElita NapiaNo ratings yet
- Basic - Concepts - in - Pharmaceutical - Care CLINICAL PHARMACYDocument17 pagesBasic - Concepts - in - Pharmaceutical - Care CLINICAL PHARMACYPrincess RonsableNo ratings yet
- Inpatient SBFRDocument14 pagesInpatient SBFRMiraf Mesfin100% (1)
- Factors Influencing Medication Non-AdherenceDocument10 pagesFactors Influencing Medication Non-AdherenceWinda WidyaNo ratings yet
- ER/ICU Journal: Organizing-Determine What Task Are To Be Done, Who Is To DoDocument3 pagesER/ICU Journal: Organizing-Determine What Task Are To Be Done, Who Is To DoWendale Claire G. ASORIONo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Management Science Associates SpdsDocument64 pagesManagement Science Associates SpdsAshwinNo ratings yet
- Defining and Implementing Value-Based Health Care - A Strategic FrameworkDocument4 pagesDefining and Implementing Value-Based Health Care - A Strategic FrameworkQuang Danh PhạmNo ratings yet
- Test Bank For Pediatric Nursing The Critical Components of Nursing Care 2nd Edition Kathryn Rudd Diane Kocisko 36Document15 pagesTest Bank For Pediatric Nursing The Critical Components of Nursing Care 2nd Edition Kathryn Rudd Diane Kocisko 36Raymond Robey100% (29)
- Evo IQ SYR CE Mark TGA Release FINALBAXTER-2021Document4 pagesEvo IQ SYR CE Mark TGA Release FINALBAXTER-2021juan alberto florez coteNo ratings yet
- Dokumen - Pub Guidebook of Somatic Transformational ExercisesDocument196 pagesDokumen - Pub Guidebook of Somatic Transformational ExercisesNuria100% (2)
- CB Insights - Healthcare Consumerization Briefing PDFDocument105 pagesCB Insights - Healthcare Consumerization Briefing PDFbandarumanasa100% (2)
- JurnalDocument16 pagesJurnalNurul RiskiNo ratings yet
- Susy PPT - Road Map To AccreditationDocument86 pagesSusy PPT - Road Map To AccreditationSUSANTONo ratings yet
- Delhi High Court Judgment On Illegal Detention in Mental HospitalDocument87 pagesDelhi High Court Judgment On Illegal Detention in Mental HospitalLatest Laws TeamNo ratings yet
- Nursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The ExperiencingDocument13 pagesNursing Diagnosis: Acute Pain: NANDA Definition: Pain Is Whatever The Experiencingasmika danaNo ratings yet
- Journal SepsisDocument8 pagesJournal Sepsisarif21492No ratings yet
- Assignment 1&2Document4 pagesAssignment 1&2nasreen modyNo ratings yet
- Patient Charter-DMAI NABHDocument3 pagesPatient Charter-DMAI NABHMoin MedicansNo ratings yet
- Jurnal OsteoartritisDocument6 pagesJurnal OsteoartritisMeong Even0% (1)
- Phlebotomist Labelling Primary Blood Tubes For Clinical Laboratory Tests An Important Step To Medical Diagnostics 2167 0870.1000e111 PDFDocument2 pagesPhlebotomist Labelling Primary Blood Tubes For Clinical Laboratory Tests An Important Step To Medical Diagnostics 2167 0870.1000e111 PDFLevi GasparNo ratings yet