You might also like
- Diskusi Kasus Resusitasi NeonatusDocument18 pagesDiskusi Kasus Resusitasi NeonatusIngrid Maria KNo ratings yet
- Diskusi Kasus Resusitasi NeonatusDocument18 pagesDiskusi Kasus Resusitasi NeonatusFuzti FauziaNo ratings yet
- Apgar Score Description PDFDocument1 pageApgar Score Description PDFAira Shane MargesNo ratings yet
- Apgar Score: Blue / Pale Pink: Extremities Blue Completely PinkDocument1 pageApgar Score: Blue / Pale Pink: Extremities Blue Completely PinkSalman KhanNo ratings yet
- Apgar ScoreDocument1 pageApgar ScoremalikrezaNo ratings yet
- APGAR Score PDFDocument1 pageAPGAR Score PDFDwi WardaniNo ratings yet
- Apgar Score: in 1953 American Anesthesiologist Virginia ApgarDocument3 pagesApgar Score: in 1953 American Anesthesiologist Virginia ApgarDian Permana BurlandNo ratings yet
- What Is The Apgar ScoreDocument2 pagesWhat Is The Apgar ScoreCherry May Soriano100% (1)
- APGAR Scoring System: Infant CareDocument8 pagesAPGAR Scoring System: Infant CareFelaih Binasoy Dela CruzNo ratings yet
- Apgar Scoring ActivityDocument3 pagesApgar Scoring ActivityAshley SorgenNo ratings yet
- Apgar ScoreDocument11 pagesApgar Scorefaizura100% (1)
- Apgar ScoringDocument5 pagesApgar ScoringMarko QuebralNo ratings yet
- Apgar ScoringDocument1 pageApgar ScoringAmoroso, Marian Corneth D.No ratings yet
- Apgar ScoringDocument9 pagesApgar Scoringkristel LudangcoNo ratings yet
- HA2Document3 pagesHA2nezukonez81No ratings yet
- Medical Procedures Checklist: APGAR ScoreDocument1 pageMedical Procedures Checklist: APGAR ScoreJaison JohnNo ratings yet
- Medical Procedures Checklist: APGAR ScoreDocument1 pageMedical Procedures Checklist: APGAR ScoreJaison JohnNo ratings yet
- Medical Procedures Checklist: APGAR ScoreDocument1 pageMedical Procedures Checklist: APGAR ScoreLerma PagcaliwanganNo ratings yet
- Nursing - CS - Newborn Apgar Scores and Implications - 04 PDFDocument1 pageNursing - CS - Newborn Apgar Scores and Implications - 04 PDFFattimah AndangNo ratings yet
- Apgar DRDocument2 pagesApgar DRJb RosillosaNo ratings yet
- Kegawatan Pada Neonatus: Diskusi KasusDocument18 pagesKegawatan Pada Neonatus: Diskusi KasusIngrid Maria KNo ratings yet
- Neurological Observation Chart A3 Spreads - Layout 1Document2 pagesNeurological Observation Chart A3 Spreads - Layout 1Arun C RajNo ratings yet
- Pain Assessment and Re AssessmentDocument1 pagePain Assessment and Re AssessmentJusmine Rose MundaNo ratings yet
- Pain Assessment and Re AssessmentDocument1 pagePain Assessment and Re AssessmentJusmine Rose MundaNo ratings yet
- Pain Assessment and Re AssessmentDocument1 pagePain Assessment and Re AssessmentNikki Batenga BonifacioNo ratings yet
- 0 1 2 Heart Rate: Absent 100 BPMDocument2 pages0 1 2 Heart Rate: Absent 100 BPMRoelleneL.No ratings yet
- Pulse Grimace Activity Respiration: 2 1 0 1 Min 5 MinDocument2 pagesPulse Grimace Activity Respiration: 2 1 0 1 Min 5 Minapi-384858632No ratings yet
- CAM ICU PocketCards PDFDocument2 pagesCAM ICU PocketCards PDFFikriNo ratings yet
- Indicator 0 1 2 A Activity P Pulse G Grimace A Appearance R RespirationDocument1 pageIndicator 0 1 2 A Activity P Pulse G Grimace A Appearance R RespirationLean CruzNo ratings yet
- Material Vincent M (APGAR Scoring)Document3 pagesMaterial Vincent M (APGAR Scoring)Vincent Maralit MaterialNo ratings yet
- Score 0 Score 1 Score 2: Blue Pale Body - Pink Extremities - Blue Completely Pink Absent Below 100 Over 100Document3 pagesScore 0 Score 1 Score 2: Blue Pale Body - Pink Extremities - Blue Completely Pink Absent Below 100 Over 100Vincent Maralit MaterialNo ratings yet
- Assessment Baby BookDocument9 pagesAssessment Baby BookWyeth Earl Padar EndrianoNo ratings yet
- START Triage: Respirations PerfusionDocument2 pagesSTART Triage: Respirations PerfusionCharlene Grace ReginoNo ratings yet
- Apgar Scoring: Birth To Ascertain The Need For Immediate CareDocument3 pagesApgar Scoring: Birth To Ascertain The Need For Immediate CarejeromeNo ratings yet
- SOPs For Medical EmergenciesDocument4 pagesSOPs For Medical EmergenciesIbrar HumayunNo ratings yet
- Triage of Adult PatientsDocument1 pageTriage of Adult PatientsjapiedtNo ratings yet
- Adult TEWS - Sheet1Document1 pageAdult TEWS - Sheet1Sivakumar GoundenNo ratings yet
- COMFORT ScaleDocument7 pagesCOMFORT ScaleALDO STEFANUZ (STIK)No ratings yet
- Sedation Pain AlgorithmDocument1 pageSedation Pain Algorithmdamondouglas100% (2)
- AC FormulaDocument2 pagesAC FormulaStopBarkingNo ratings yet
- Preeclampsia Early Recognition ToolDocument1 pagePreeclampsia Early Recognition ToolHaniv Prasetya AdhiNo ratings yet
- Icu 101Document1 pageIcu 101Liga Medicina InternaNo ratings yet
- FLACC Pain Assessment Scale 1 PDFDocument1 pageFLACC Pain Assessment Scale 1 PDFLucia NatashaNo ratings yet
- FLAACDocument4 pagesFLAACNaser MuhammadNo ratings yet
- Clinical SkillsDocument1 pageClinical SkillsjamiescuffellNo ratings yet
- Glasgow Coma ScaleDocument4 pagesGlasgow Coma ScaleRajveer100% (1)
- Head To Toe Assessment Guide PDFDocument6 pagesHead To Toe Assessment Guide PDFTashaNo ratings yet
- Glasgow Coma ScaleDocument1 pageGlasgow Coma ScaleLara Marie MACALINTALNo ratings yet
- Neuro Observation SheetDocument2 pagesNeuro Observation SheetJamaica LimejuiceNo ratings yet
- PFD Pain Assessment CE GrossDocument24 pagesPFD Pain Assessment CE GrossAndrew TimantaNo ratings yet
- Sign 0 1 2 Appearance Pulse GrimaceDocument2 pagesSign 0 1 2 Appearance Pulse GrimaceChum ChitaruNo ratings yet
- Maryland Triage System: Tag, Start, and JumpstartDocument39 pagesMaryland Triage System: Tag, Start, and JumpstartmiraNo ratings yet
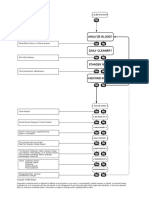
- Flow Chart: Analyze Blood?Document1 pageFlow Chart: Analyze Blood?Dialife Medical Equipment and Supplies0% (1)
- Date Time: (24 Hour) : Adult Vital Signs ChartDocument9 pagesDate Time: (24 Hour) : Adult Vital Signs ChartEmma NuroNo ratings yet
- Aspire User GuideDocument8 pagesAspire User GuideJose Luis DorronsoroNo ratings yet
- ScoringDocument1 pageScoringjennyNo ratings yet
- Pediatric AssessmentDocument5 pagesPediatric AssessmentmitchNo ratings yet
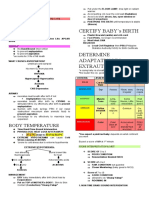
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Format Ujian KomterDocument1 pageFormat Ujian Komterteti kurniatiNo ratings yet
- Daftar Dinas Bulan NovemberDocument1 pageDaftar Dinas Bulan Novemberteti kurniatiNo ratings yet
- Daftar Dinas Bulan NovemberDocument1 pageDaftar Dinas Bulan Novemberteti kurniatiNo ratings yet
- Daftar Dinas Bulan NovemberDocument1 pageDaftar Dinas Bulan Novemberteti kurniatiNo ratings yet
- OT6 - Valsalva ManeuverDocument7 pagesOT6 - Valsalva ManeuverAnnbe BarteNo ratings yet
- Final Result of PG 2022 Special Stray Vacancy RounDocument43 pagesFinal Result of PG 2022 Special Stray Vacancy Rounu19n6735No ratings yet
- Em Form NktiDocument7 pagesEm Form NktiJerico Wendell Gee RubioNo ratings yet
- 3100A HFOV BrochureDocument4 pages3100A HFOV BrochureSwami MeeraNo ratings yet
- Nicu Checklist Bundles Infection Control 1Document60 pagesNicu Checklist Bundles Infection Control 1Mithlesh Dewangan92% (13)
- Placenta PreviaDocument8 pagesPlacenta PreviaBj DuquesaNo ratings yet
- Medicolegal ProblemsDocument2 pagesMedicolegal ProblemsBabith Moses WilbyNo ratings yet
- Biologic Basis Tooth Movement-Ortho / Orthodontic Courses by Indian Dental AcademyDocument47 pagesBiologic Basis Tooth Movement-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- A Night at The Museum: Roll Up ! Roll Up! Museums IncDocument1 pageA Night at The Museum: Roll Up ! Roll Up! Museums IncKeeranmayeeishraNo ratings yet
- Pediatric Nursing Practice TestDocument10 pagesPediatric Nursing Practice TestEthel Gretchen Casalla71% (7)
- Git MotilityDocument68 pagesGit MotilityGaurav SinghNo ratings yet
- Two-Way Referral Form PDFDocument1 pageTwo-Way Referral Form PDFcatherine joy macalos100% (4)
- Behavior Guidance For The Pediatric Dental Patient: Latest RevisionDocument14 pagesBehavior Guidance For The Pediatric Dental Patient: Latest RevisionEnrita DianNo ratings yet
- Philiphs HD7 Brochure - UltrasoundDocument6 pagesPhiliphs HD7 Brochure - UltrasoundIvan CvasniucNo ratings yet
- James Brazelle Res OtaDocument4 pagesJames Brazelle Res Otaapi-300158819No ratings yet
- Malinda Richards: Pioneer For Nurse Education First American Trained NurseDocument25 pagesMalinda Richards: Pioneer For Nurse Education First American Trained Nursejls038100% (1)
- RAH MapDocument1 pageRAH Maptravis_izNo ratings yet
- The Prevention and Management of Congenital SyphilDocument10 pagesThe Prevention and Management of Congenital Syphillink_wolfloboNo ratings yet
- Zirconnia Knife Edge PDFDocument6 pagesZirconnia Knife Edge PDFMuaiyed Buzayan AkremyNo ratings yet
- Voluson S Series - Transducer Guide (En)Document2 pagesVoluson S Series - Transducer Guide (En)Zákány ZoltánNo ratings yet
- How Does Hypnosis WorkDocument11 pagesHow Does Hypnosis WorkchoileoNo ratings yet
- Eng - PB 2016 FinalDocument6 pagesEng - PB 2016 Finalashok PradhanNo ratings yet
- HPCZ Application FormDocument11 pagesHPCZ Application FormQualis LabsNo ratings yet
- Dental Hygiene ResumeDocument2 pagesDental Hygiene Resumeapi-663723303No ratings yet
- Spine ConfDocument5 pagesSpine ConfVivek PatilNo ratings yet
- Monobind CatalogDocument37 pagesMonobind CatalogRobert Caballero Bardales100% (2)
- Monteggia FractureDocument11 pagesMonteggia FractureRonald Ivan WijayaNo ratings yet
- A To Z Orthodontics MCQDocument112 pagesA To Z Orthodontics MCQUjjwal Pyakurel100% (4)
- Types of Rickets: Annals of Orthopedics & RheumatologyDocument6 pagesTypes of Rickets: Annals of Orthopedics & RheumatologyNadejda MarcovaNo ratings yet
- Guías Infecciones Asociadas A Cateter IDSA 2009Document45 pagesGuías Infecciones Asociadas A Cateter IDSA 2009pablocaballiniNo ratings yet