You might also like
- Obstetrics and Gynecology Question PapersDocument22 pagesObstetrics and Gynecology Question Papersprinceej83% (18)
- AnthraxDocument20 pagesAnthraxanemenyee100% (2)
- Bacteriology PDFDocument49 pagesBacteriology PDFPearl Medina100% (2)
- Maintenance Scheduling For Electrical EquipmentDocument82 pagesMaintenance Scheduling For Electrical Equipmentduonza100% (6)
- Practical Research 2 Quarter 1 Activity SheetsDocument8 pagesPractical Research 2 Quarter 1 Activity SheetsJonnis Estillore100% (1)
- Carlin Smith Child Abuse FinalDocument12 pagesCarlin Smith Child Abuse FinalCarlin SmithNo ratings yet
- .Class BacillusDocument38 pages.Class BacillusManoj KumarNo ratings yet
- AnthraxDocument20 pagesAnthraxanemenyeeNo ratings yet
- AnthraxDocument20 pagesAnthraxaristadevyaNo ratings yet
- Bacillus anthracis: The Cause of AnthraxDocument20 pagesBacillus anthracis: The Cause of AnthraxRizky Bayu AjieNo ratings yet
- Clostridia and Bacillus Lecture NotesDocument37 pagesClostridia and Bacillus Lecture NotesPrincewill SeiyefaNo ratings yet
- Gram-Positive Bacilli of Medical Importance IDocument87 pagesGram-Positive Bacilli of Medical Importance IJoeyNo ratings yet
- MicrobiologyDocument63 pagesMicrobiologyBhaski MadhappanNo ratings yet
- Lec 15mycology SPPDocument35 pagesLec 15mycology SPPbujalkanNo ratings yet
- Domai N Phylu M Class Order Family Genus Specie S: SystematicsDocument14 pagesDomai N Phylu M Class Order Family Genus Specie S: SystematicsVedha VincyNo ratings yet
- Am Positive Rods-1Document73 pagesAm Positive Rods-1temesgensemahegn55No ratings yet
- Bacillus Species Characteristics and Medically Important TypesDocument31 pagesBacillus Species Characteristics and Medically Important TypesNaing Lin SoeNo ratings yet
- 3.1. Gram Positive Rods-BacillusDocument32 pages3.1. Gram Positive Rods-Bacillusahmed mohammedNo ratings yet
- 10 Bacillus & ClostridiumDocument11 pages10 Bacillus & ClostridiumASECO LISHNo ratings yet
- Bacillus Species Classification and CharacteristicsDocument47 pagesBacillus Species Classification and CharacteristicsAnonymous rzPX6lUNo ratings yet
- Bacillus Anthracis: Hirotaka Ishibashi Jennifer Jolivet Sean Patrick KellyDocument92 pagesBacillus Anthracis: Hirotaka Ishibashi Jennifer Jolivet Sean Patrick KellyReyza HasnyNo ratings yet
- Filariasis and Hookworm DiseaseDocument97 pagesFilariasis and Hookworm DiseaseHarton MuhammadNo ratings yet
- Basic MicrobiologyDocument53 pagesBasic MicrobiologyJohn NirmalNo ratings yet
- Micro by DR - Hesham (GIT)Document65 pagesMicro by DR - Hesham (GIT)abcde990075No ratings yet
- Rahul KambleDocument5 pagesRahul KambleAnonymous 6EHECZNo ratings yet
- General Pathology of Infectious DiseasesDocument42 pagesGeneral Pathology of Infectious Diseasesapi-19916399No ratings yet
- Livestock Diseases 1: Bovine Mastitis and AnthraxDocument108 pagesLivestock Diseases 1: Bovine Mastitis and AnthraxchachaNo ratings yet
- Bacillus Anthracis PowerpointDocument32 pagesBacillus Anthracis PowerpointEnerose MagnoNo ratings yet
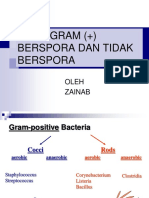
- Spore Forming Gram Positive Bacteria: Prof. Zainab A AldhaherDocument17 pagesSpore Forming Gram Positive Bacteria: Prof. Zainab A Aldhaherمروه عماد عيسىNo ratings yet
- P3 Basil Gram (+) Rev2016Document50 pagesP3 Basil Gram (+) Rev2016AuliaNo ratings yet
- Bacillus Anthracis Microbilogy LectureDocument40 pagesBacillus Anthracis Microbilogy Lecturepodcast gazalNo ratings yet
- Faculty of Medicine Hashemite University DR Mohammad Al-Tamimi, MD, Master Biomed, PHDDocument46 pagesFaculty of Medicine Hashemite University DR Mohammad Al-Tamimi, MD, Master Biomed, PHDDaniel AtiehNo ratings yet
- Bacteriology by Dhshan Hassan DhshanDocument48 pagesBacteriology by Dhshan Hassan Dhshanعلي الكوافي100% (1)
- Microbiology Module 7 - BacilliDocument87 pagesMicrobiology Module 7 - BacilliArt Arts100% (1)
- Symbiotic Relations and Microbes Normal MicrofloreDocument32 pagesSymbiotic Relations and Microbes Normal MicrofloreAndulile Francis MwaigwisyaNo ratings yet
- (PROTOZOANS) Phylum ApicomplexaDocument8 pages(PROTOZOANS) Phylum ApicomplexaEunice AndradeNo ratings yet
- LMRDocument15 pagesLMR8b8xppmgpcNo ratings yet
- TRANS GROUP 2Document8 pagesTRANS GROUP 2Alanah JaneNo ratings yet
- Anthrax ReaserchDocument17 pagesAnthrax Reaserchsozakarem35No ratings yet
- Introduction To Biotechnology - Pharmaceutical Application - 2021Document68 pagesIntroduction To Biotechnology - Pharmaceutical Application - 2021Dương Hà Trúc TâmNo ratings yet
- Multiple Species: Section 2.1Document10 pagesMultiple Species: Section 2.1WormInchNo ratings yet
- Soal Ujian Akhir MycologyDocument6 pagesSoal Ujian Akhir Mycologygan_asaNo ratings yet
- W6 PresentationDocument72 pagesW6 PresentationUkash sukarmanNo ratings yet
- Bacteria TableDocument4 pagesBacteria TableBrittany Lynn MyersNo ratings yet
- Chlamydia & MycoplasmaDocument6 pagesChlamydia & MycoplasmaLuqman Al-Bashir FauziNo ratings yet
- TOXOPLASMOSISDocument31 pagesTOXOPLASMOSISVenkatapradeepNo ratings yet
- ANTHRAXDocument44 pagesANTHRAXjeevan ghimireNo ratings yet
- Session 3 PathogenesisDocument18 pagesSession 3 Pathogenesisannelle0219No ratings yet
- Peran Mikroorganisme Dalam Kehidupan-2Document51 pagesPeran Mikroorganisme Dalam Kehidupan-2Safhira Nur HidayatiNo ratings yet
- Cabison - Mycology ReviewerDocument10 pagesCabison - Mycology ReviewerPatricia Cabison100% (1)
- Microb KARDIO 2019Document48 pagesMicrob KARDIO 2019sintia djafarNo ratings yet
- 5 CorynebacteriumDocument41 pages5 Corynebacterium01. Akhmad Gilang R - XII MIPA 4No ratings yet
- Antimicrobial Susceptibility in ThermophilicCampylobacterspecies Isolatedfrom Pigs and Chickens in South AfricaDocument9 pagesAntimicrobial Susceptibility in ThermophilicCampylobacterspecies Isolatedfrom Pigs and Chickens in South AfricanigeldkdcNo ratings yet
- Common Skin and Soft Tissue InfectionsDocument8 pagesCommon Skin and Soft Tissue InfectionsAdel mohammadNo ratings yet
- AnthraxDocument29 pagesAnthraxstevensb055No ratings yet
- Animal Experiments in Medical MicrobiologyDocument70 pagesAnimal Experiments in Medical Microbiologyira_praharaj100% (3)
- PseudomiseliumDocument6 pagesPseudomiseliumRisma Karimah PratiwiNo ratings yet
- 2020 Bacillus Power Point Voice TaggedDocument42 pages2020 Bacillus Power Point Voice Taggedkrisk990322No ratings yet
- Medical Mycology Arthur F. Di Salvo, MD Reno, NevadaDocument124 pagesMedical Mycology Arthur F. Di Salvo, MD Reno, Nevadablue_blooded23No ratings yet
- Opportunistic MycosesDocument3 pagesOpportunistic MycosesZarah Mae InghugNo ratings yet
- Nematodes LabDocument57 pagesNematodes LabAlaa ZiyadNo ratings yet
- Miraña Genus AeromonasDocument1 pageMiraña Genus AeromonasAlmira Joy MirañaNo ratings yet
- Advantages/Benefits of OOP 1. Re-UsabilityDocument2 pagesAdvantages/Benefits of OOP 1. Re-Usabilityjamal nasirNo ratings yet
- PseudomonasDocument42 pagesPseudomonasjamal nasirNo ratings yet
- Weekwise Lecture Plan-VP-MCSDocument3 pagesWeekwise Lecture Plan-VP-MCSjamal nasir100% (1)
- Weekwise Lecture Plan-VP-MCSDocument3 pagesWeekwise Lecture Plan-VP-MCSjamal nasir100% (1)
- StaphDocument40 pagesStaphjamal nasirNo ratings yet
- Computer Basics: An Introduction To Computer HardwareDocument10 pagesComputer Basics: An Introduction To Computer Hardwarejamal nasirNo ratings yet
- OOP (Object Oriented Programming)Document16 pagesOOP (Object Oriented Programming)jamal nasirNo ratings yet
- DotNetFramework VSDocument36 pagesDotNetFramework VSjamal nasirNo ratings yet
- Visual Programming: Muhammad Ahmad JanDocument41 pagesVisual Programming: Muhammad Ahmad Janjamal nasirNo ratings yet
- Chapter 01Document45 pagesChapter 01Ahsen KhanNo ratings yet
- Computer Security: Jamal A NasirDocument13 pagesComputer Security: Jamal A Nasirjamal nasirNo ratings yet
- PseudomonasDocument42 pagesPseudomonasjamal nasirNo ratings yet
- Computer Network: Jamal A NasirDocument11 pagesComputer Network: Jamal A Nasirjamal nasirNo ratings yet
- Artificial IntelligenceDocument16 pagesArtificial Intelligencejamal nasirNo ratings yet
- YersiniaDocument46 pagesYersiniajamal nasir50% (2)
- Viruses IntroductionDocument48 pagesViruses Introductionjamal nasir100% (1)
- Course Allocation September 2018Document2 pagesCourse Allocation September 2018jamal nasirNo ratings yet
- Pathogenesis of Bacterial Infection WebDocument35 pagesPathogenesis of Bacterial Infection Webjamal nasirNo ratings yet
- Clostrdia: G Positive Spore Forming Anaerobic Toxin Producing RodsDocument36 pagesClostrdia: G Positive Spore Forming Anaerobic Toxin Producing Rodsjamal nasirNo ratings yet
- Zoonosis: A Disease Primarily of Animals Which Can Be Transmitted To Man Directly or Indirectly From Infected AnimalDocument25 pagesZoonosis: A Disease Primarily of Animals Which Can Be Transmitted To Man Directly or Indirectly From Infected Animaljamal nasirNo ratings yet
- Pathogenesis of Bacterial Infection WebDocument35 pagesPathogenesis of Bacterial Infection Webjamal nasirNo ratings yet
- Hemophilus & BodetellaDocument36 pagesHemophilus & Bodetellajamal nasirNo ratings yet
- Acinetobacter baumannii: A Brief Review of an Opportunistic PathogenDocument15 pagesAcinetobacter baumannii: A Brief Review of an Opportunistic Pathogenjamal nasirNo ratings yet
- Cricket basics: batting, bowling, runs, oversDocument4 pagesCricket basics: batting, bowling, runs, oversjamal nasirNo ratings yet
- 3.course Allocation Feb-2019Document3 pages3.course Allocation Feb-2019jamal nasirNo ratings yet
- Acinetobacter baumannii: A Brief Review of an Opportunistic PathogenDocument15 pagesAcinetobacter baumannii: A Brief Review of an Opportunistic Pathogenjamal nasirNo ratings yet
- MIDocument60 pagesMIjamal nasirNo ratings yet
- Cricket basics: batting, bowling, runs, oversDocument4 pagesCricket basics: batting, bowling, runs, oversjamal nasirNo ratings yet
- Cricket: 3 Semester ClassDocument4 pagesCricket: 3 Semester Classjamal nasirNo ratings yet
- Wirmen Beautycare Cloth Pad SDN - BHDDocument9 pagesWirmen Beautycare Cloth Pad SDN - BHDadilahNo ratings yet
- The Differential Diagnosis of Fluoride and Non-Fluoride OpacitiesDocument4 pagesThe Differential Diagnosis of Fluoride and Non-Fluoride OpacitiesRajshekhar BanerjeeNo ratings yet
- Email chat about sex actsDocument10 pagesEmail chat about sex actsrishav kumar agarwalNo ratings yet
- Endocrine DisruptorsDocument50 pagesEndocrine DisruptorsSnowangeleyes AngelNo ratings yet
- MDR Guideline Medical Devices LabelingDocument7 pagesMDR Guideline Medical Devices Labelingarade43100% (1)
- Week 4-Physical Fitness TestDocument38 pagesWeek 4-Physical Fitness TestCatherine Sagario OliquinoNo ratings yet
- 1866 PSC Iasc Ref Guidance t2 DigitalDocument11 pages1866 PSC Iasc Ref Guidance t2 DigitalDama BothNo ratings yet
- 0007PNTDocument11 pages0007PNTPau Lo JakobyNo ratings yet
- Anatomy of Writing For Publication For Nurses PDFDocument369 pagesAnatomy of Writing For Publication For Nurses PDFfernlover3901100% (1)
- Domestic Physician HeringDocument490 pagesDomestic Physician Heringskyclad_21No ratings yet
- 67166-Apvma Veterinary Medicines Technical Report TemplateDocument42 pages67166-Apvma Veterinary Medicines Technical Report Templateali aimanNo ratings yet
- Pneumonia Care PlanDocument1 pagePneumonia Care Plantcumurphish67% (3)
- Technology and Livelihood Education: Quarter 1 - Module 4: CaregivingDocument20 pagesTechnology and Livelihood Education: Quarter 1 - Module 4: CaregivingIrine Irine100% (1)
- Article Text Batuk EfektifDocument7 pagesArticle Text Batuk EfektifWelang 102No ratings yet
- HSE List of PublicationsDocument12 pagesHSE List of PublicationsDanijel PindrićNo ratings yet
- The Doctor-Patient Relationship and Interviewing TechniquesDocument50 pagesThe Doctor-Patient Relationship and Interviewing TechniquesPranay KumarNo ratings yet
- Hahnemann Advance MethodDocument2 pagesHahnemann Advance MethodRehan AnisNo ratings yet
- Lesson 1 Local Government's Historical BackgroundDocument16 pagesLesson 1 Local Government's Historical BackgroundLorienelNo ratings yet
- Confidence Intervals For Ratio of Two Poisson Rates Using The Method of Variance Estimates RecoveryDocument23 pagesConfidence Intervals For Ratio of Two Poisson Rates Using The Method of Variance Estimates RecoveryJaneNo ratings yet
- Sampling Methods GuideDocument35 pagesSampling Methods GuideKim RamosNo ratings yet
- Tbf-531Bodyfat Monitor/Scale: Instruction ManualDocument13 pagesTbf-531Bodyfat Monitor/Scale: Instruction ManualJose JimenoNo ratings yet
- Talisay Leaf Extract Cures Betta Fish in Less Time than Methylene BlueDocument8 pagesTalisay Leaf Extract Cures Betta Fish in Less Time than Methylene BlueMuhammad Rehan Said100% (1)
- Family Nursing Care PlanDocument1 pageFamily Nursing Care PlanDersly LaneNo ratings yet
- Manu SkripDocument20 pagesManu SkripzanimarNo ratings yet
- Ergonomics (Uu Tien Dich)Document6 pagesErgonomics (Uu Tien Dich)Phong D LeNo ratings yet
- Jha For Painting of EquipmentDocument1 pageJha For Painting of EquipmentShahid RazaNo ratings yet