You might also like
- Pepti C Ul Cer Dis Ea SeDocument36 pagesPepti C Ul Cer Dis Ea Segerald_ichigoNo ratings yet
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseasePernel Jose Alam MicuboNo ratings yet
- GastritisDocument64 pagesGastritisaparna shamaNo ratings yet
- Helicobacter Pylori: Dr.B.BoyleDocument35 pagesHelicobacter Pylori: Dr.B.BoyleTammy AdjaNo ratings yet
- Peptic UlcerDocument36 pagesPeptic Ulcersable1804No ratings yet
- Ziziphus Spina Christi20200317 4568 1vzdzos With Cover Page v2Document15 pagesZiziphus Spina Christi20200317 4568 1vzdzos With Cover Page v2Rosnidar SumardiNo ratings yet
- Gastric Pathology: Mechanisms of Mucosal Protection and DiseaseDocument49 pagesGastric Pathology: Mechanisms of Mucosal Protection and DiseaseKiara GovenderNo ratings yet
- Key Point of Gut - Kidney AxisDocument4 pagesKey Point of Gut - Kidney AxisAlfirahmatikaNo ratings yet
- Research Article Chlamydia Pneumoniae: Roquefort Cheese Proteins Inhibit Propagation and LPS-Induced Leukocyte MigrationDocument6 pagesResearch Article Chlamydia Pneumoniae: Roquefort Cheese Proteins Inhibit Propagation and LPS-Induced Leukocyte MigrationKevin Ponce DextreNo ratings yet
- Staphylococci: Streptococcus PyogenesDocument20 pagesStaphylococci: Streptococcus PyogenesPharmacy2015100% (2)
- Report On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Document3 pagesReport On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Adnan Akram, MD (Latvia)No ratings yet
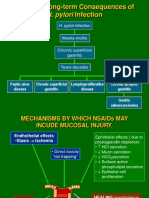
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 pagesH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaNo ratings yet
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 pagesH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaNo ratings yet
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseaseValerrie NgenoNo ratings yet
- Peptic Ulcer Disease: J. Rashma 2015 BATCHDocument16 pagesPeptic Ulcer Disease: J. Rashma 2015 BATCHRashma JosephNo ratings yet
- Etiology of Peptic Ulcer DiseaseDocument4 pagesEtiology of Peptic Ulcer Diseaseshufi100% (1)
- Hepatology - 2011 - Teltschik - Intestinal Bacterial Translocation in Rats With Cirrhosis Is Related To Compromised PanethDocument10 pagesHepatology - 2011 - Teltschik - Intestinal Bacterial Translocation in Rats With Cirrhosis Is Related To Compromised PanethAyelén GuzmánNo ratings yet
- Dietary L-Arginine Supplementation Reduces Methotrexate Induced Intestinal Mucosal Injury in RatDocument9 pagesDietary L-Arginine Supplementation Reduces Methotrexate Induced Intestinal Mucosal Injury in RatMohamed IsmailNo ratings yet
- Kuliah Modul Gi 2013Document155 pagesKuliah Modul Gi 2013ck dwnNo ratings yet
- Peptic Ulcer DiseaseDocument3 pagesPeptic Ulcer DiseaseABEL KETEMANo ratings yet
- Peptic Ulcer DiseaseDocument16 pagesPeptic Ulcer DiseaseRashma JosephNo ratings yet
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDocument82 pagesGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- Lect - Peptic Ulcer - 211020 - 182113Document38 pagesLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelNo ratings yet
- 10.3934 Microbiol.2022035Document22 pages10.3934 Microbiol.2022035Leila HashimotoNo ratings yet
- Signals in Spoilage of Bean Sprouts Involvement of Bacterial Quorum-SensingDocument11 pagesSignals in Spoilage of Bean Sprouts Involvement of Bacterial Quorum-SensingKothari VishalNo ratings yet
- Gastritis: Palangka Raya University Faculty of MedicineDocument32 pagesGastritis: Palangka Raya University Faculty of MedicineAnonymNo ratings yet
- Helicobacter pylori Risk Factors and Clinical ManifestationsDocument2 pagesHelicobacter pylori Risk Factors and Clinical ManifestationsNeil AlviarNo ratings yet
- Carotene and Lutein Inhibit Hydrogen Peroxide-Induced Activation of NF-B and IL-8 Expression in Gastric Epithelial AGS CellsDocument8 pagesCarotene and Lutein Inhibit Hydrogen Peroxide-Induced Activation of NF-B and IL-8 Expression in Gastric Epithelial AGS Cellsnaziva annisaNo ratings yet
- Sepsis Induced CholestasisDocument12 pagesSepsis Induced CholestasisYusuf Hakim AjiNo ratings yet
- PSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionDocument7 pagesPSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionMichael TobilobaNo ratings yet
- R4. 2020 Critical Reviews in OncogenesisDocument14 pagesR4. 2020 Critical Reviews in OncogenesissathishNo ratings yet
- Stomach PathologyDocument45 pagesStomach PathologytahaNo ratings yet
- Julia Nur Faridha SDocument9 pagesJulia Nur Faridha SJulia Nur Faridha SeptyaniNo ratings yet
- Tumor Necrosis Factor-A-Induced Colitis IncreasesDocument15 pagesTumor Necrosis Factor-A-Induced Colitis IncreasesSalma MehafdiNo ratings yet
- GIT 1 - StomachDocument45 pagesGIT 1 - StomachHussain SafaaNo ratings yet
- Clinical Bacteriology by DR Agwu EzeraDocument116 pagesClinical Bacteriology by DR Agwu EzeraRodgers Bazigu100% (1)
- Research Progress On Traditional Chinese Medicine Regulating Gut Microbiota in Treatment of Chronic DiarrheaDocument11 pagesResearch Progress On Traditional Chinese Medicine Regulating Gut Microbiota in Treatment of Chronic Diarrheanguyen thaiNo ratings yet
- Inflammatory Bowel DiseaseDocument35 pagesInflammatory Bowel DiseaseMpanso Ahmad AlhijjNo ratings yet
- Enfermedad Ácido-PépticaDocument10 pagesEnfermedad Ácido-PépticaDoris Santiago FloresNo ratings yet
- Antiulcer Activity of Natural Compounds: A Review: Issn 0975-2331 (Print) 0975-4385 (Online)Document7 pagesAntiulcer Activity of Natural Compounds: A Review: Issn 0975-2331 (Print) 0975-4385 (Online)maria ulfahNo ratings yet
- Bakteri, Virus dan Penyakit Gastrointestinal (2Document52 pagesBakteri, Virus dan Penyakit Gastrointestinal (2ilhamNo ratings yet
- Peptic Ulcer Disease: GastrologyDocument14 pagesPeptic Ulcer Disease: GastrologyMarie Jennifer ParilNo ratings yet
- Presentation FucoidanDocument42 pagesPresentation FucoidanTaufik Akbar Faried LubisNo ratings yet
- 1 s2.0 S0006295223002642 MainDocument15 pages1 s2.0 S0006295223002642 Main吴善统No ratings yet
- Everything You Need to Know About GastritisDocument86 pagesEverything You Need to Know About Gastritisindri damayantiNo ratings yet
- Polysaccharide from Scutellaria baicalensis Georgi ameliorates colitis via suppressing NF-κB signaling and NLRP3 inflammasome activationDocument13 pagesPolysaccharide from Scutellaria baicalensis Georgi ameliorates colitis via suppressing NF-κB signaling and NLRP3 inflammasome activationMartinaNo ratings yet
- Micro Chapter 17Document8 pagesMicro Chapter 17Ana AbuladzeNo ratings yet
- Duodenal Ulcer Risk FactorsDocument3 pagesDuodenal Ulcer Risk FactorsJanelle BondadNo ratings yet
- Anti Infection AgentsDocument18 pagesAnti Infection AgentsRawabi SalehNo ratings yet
- Effects of Different Probiotic Strains of Lactobacillus and Acute Liver Injury ModelDocument8 pagesEffects of Different Probiotic Strains of Lactobacillus and Acute Liver Injury ModelNofiyanty NicolasNo ratings yet
- The Gut Brain ConnectionDocument33 pagesThe Gut Brain ConnectionRia RahmawatiNo ratings yet
- Francisco G. La Rosa, M.D.: Pancreas Pathology and Diabetes Mellitus (Course Dsbs 5516)Document10 pagesFrancisco G. La Rosa, M.D.: Pancreas Pathology and Diabetes Mellitus (Course Dsbs 5516)madaniNo ratings yet
- Review Article Helicobacter Pylori-Induced Chronic Gastritis andDocument9 pagesReview Article Helicobacter Pylori-Induced Chronic Gastritis andGwpengenlohthao Gwknslalusyankmalo MskilodaggsyankmagwNo ratings yet
- GRAM Positive CocciDocument67 pagesGRAM Positive CocciNoraine Princess TabangcoraNo ratings yet
- 1-s2.0-S0022316622004588-mainDocument11 pages1-s2.0-S0022316622004588-mainNejc KovačNo ratings yet
- Abdominal Surgery All in OneDocument50 pagesAbdominal Surgery All in OneAnne ChoyNo ratings yet
- Peptic Ulcer DiseaseDocument63 pagesPeptic Ulcer DiseaseAliNo ratings yet
- Peptic Ulcer Disease and Related Disorders ExplainedDocument50 pagesPeptic Ulcer Disease and Related Disorders Explainednathan asfahaNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- The Toxicology of Aflatoxins: Human Health, Veterinary, and Agricultural SignificanceFrom EverandThe Toxicology of Aflatoxins: Human Health, Veterinary, and Agricultural SignificanceDavid L. EatonNo ratings yet
- Bridger - Some Fundamental Aspects of Posture Related To Ergonomics PDFDocument13 pagesBridger - Some Fundamental Aspects of Posture Related To Ergonomics PDFEduardo DiestraNo ratings yet
- University of Madras Syllabus for Softskills CoursesDocument33 pagesUniversity of Madras Syllabus for Softskills Coursesseema sweetNo ratings yet
- DLSU A Plastic Ocean Reaction PaperDocument2 pagesDLSU A Plastic Ocean Reaction PaperJued Cisneros100% (1)
- Biocomputers: Using Biological Systems to Perform Computational CalculationsDocument3 pagesBiocomputers: Using Biological Systems to Perform Computational CalculationsAjinkyaJadNo ratings yet
- Disease Detectives B-Answer KeyDocument14 pagesDisease Detectives B-Answer KeyskdfkjlNo ratings yet
- 6177-Article Text-39080-1-10-20160922Document14 pages6177-Article Text-39080-1-10-20160922Fadlika AhmadiNo ratings yet
- Enzymes: Non-Starch Polysaccharides (NSP)Document6 pagesEnzymes: Non-Starch Polysaccharides (NSP)amamùra maamarNo ratings yet
- Biology HL Student GuideDocument134 pagesBiology HL Student GuideYesenia JassoNo ratings yet
- R Gupta Popular Master Guide For CUET-UG Biology 2022Document101 pagesR Gupta Popular Master Guide For CUET-UG Biology 2022Somya KulshresthaNo ratings yet
- Revised NEET XI Online Test GridDocument2 pagesRevised NEET XI Online Test Gridsanoojuv783105No ratings yet
- English CG (GR 7-8)Document17 pagesEnglish CG (GR 7-8)Rebell Mutya TanNo ratings yet
- Reading comprehension passages for live classDocument3 pagesReading comprehension passages for live classkuydutiknNo ratings yet
- Ultrasonic Liposuction Unit ManualDocument9 pagesUltrasonic Liposuction Unit ManualDaniel MaldonadoNo ratings yet
- DNS A InstructionsDocument2 pagesDNS A InstructionsWilda PanjaitanNo ratings yet
- Merda SeccaDocument25 pagesMerda Seccamothafukka100% (5)
- The Good DoctorDocument5 pagesThe Good DoctorDr MalazNo ratings yet
- X Science QPDocument7 pagesX Science QPhritikaray4475No ratings yet
- A United-Residue Force Field For Off-Lattice Protein-Structure Simulations. I. Functional Forms and Parameters of Long-Range Side-Chain Interaction Potentials From Protein Crystal DataDocument25 pagesA United-Residue Force Field For Off-Lattice Protein-Structure Simulations. I. Functional Forms and Parameters of Long-Range Side-Chain Interaction Potentials From Protein Crystal DataAssem AbozeedNo ratings yet
- 2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerDocument14 pages2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerFede0No ratings yet
- Raven Biology of Plants: Eighth EditionDocument41 pagesRaven Biology of Plants: Eighth EditionMoath EnnabNo ratings yet
- CBSE Class 9 Biology The Fundamental Unit of LifeDocument3 pagesCBSE Class 9 Biology The Fundamental Unit of Lifeaaditya100% (1)
- Balaytigue National High SchoolDocument2 pagesBalaytigue National High School3 stacksNo ratings yet
- 0000 Evaluation of Herbaceous Perennials As WeedDocument7 pages0000 Evaluation of Herbaceous Perennials As WeedManda ManuelaNo ratings yet
- MICRO Lecture 1 Introduction To Microbiology and Parasitology 1 PDFDocument29 pagesMICRO Lecture 1 Introduction To Microbiology and Parasitology 1 PDFJireh AcabalNo ratings yet
- Barrons Essential 800 WordsDocument12 pagesBarrons Essential 800 WordsZaheer Abbas100% (1)
- Patau SindromDocument4 pagesPatau SindromOgnjen IvkovićNo ratings yet
- Mini-CLIA SystemDocument6 pagesMini-CLIA SystemVictoria AnnaNo ratings yet
- Bet Question Paper 2008Document24 pagesBet Question Paper 2008Vasu MathuraNo ratings yet
- Science 10 Activities Weeks 7 and 8Document11 pagesScience 10 Activities Weeks 7 and 8Kim CamposanoNo ratings yet
- Major Histocompatibility Complex Part 1 TranscriptDocument24 pagesMajor Histocompatibility Complex Part 1 Transcriptapi-273068056No ratings yet