You might also like
- Major ConnectorsDocument29 pagesMajor Connectorssanaa_yadavNo ratings yet
- Amino Acid PDFDocument3 pagesAmino Acid PDFGio RiveraNo ratings yet
- Parts & Design of RPDDocument18 pagesParts & Design of RPDR KaranNo ratings yet
- Chapter 17 - ElectrochemistryDocument3 pagesChapter 17 - ElectrochemistryrNo ratings yet
- Antibiotic Break Down ChartDocument4 pagesAntibiotic Break Down ChartBram StokerNo ratings yet
- WordsDocument7 pagesWordsChelsey SchlembachNo ratings yet
- ProsthodonticsDocument280 pagesProsthodonticssavNo ratings yet
- Review of Selected Topics in Removable ProsthodonticsDocument144 pagesReview of Selected Topics in Removable ProsthodonticsneeNo ratings yet
- Components of Removable Partial Denture Prostheses-Dr - PaulamiDocument35 pagesComponents of Removable Partial Denture Prostheses-Dr - PaulamiVincent SerNo ratings yet
- Protein Chemistry: Dr. B.Divya Dharshini Department of BiochemistryDocument57 pagesProtein Chemistry: Dr. B.Divya Dharshini Department of BiochemistryTasneem AhmedNo ratings yet
- Notes IELTSDocument90 pagesNotes IELTSParth MehtaNo ratings yet
- Access Cavity Preparation FinalDocument63 pagesAccess Cavity Preparation Finalrasagna reddyNo ratings yet
- Oral Biology Lecture TopicsDocument6 pagesOral Biology Lecture TopicsMuhamad Andika Arief PutranamiNo ratings yet
- ArticulatorsDocument52 pagesArticulatorsBharath KondaveetiNo ratings yet
- Major CONNECTORS in RPDDocument73 pagesMajor CONNECTORS in RPDreem eltyebNo ratings yet
- Pulpo, Pulpec, Apex, Injuries 1Document6 pagesPulpo, Pulpec, Apex, Injuries 1Cyril Almario Cunanan100% (1)
- Introduction To Oral HistologyDocument30 pagesIntroduction To Oral HistologyShalini NairNo ratings yet
- Mandibular MovementsDocument36 pagesMandibular MovementsRagini ShravanNo ratings yet
- Muscles of Mastication: - DR - Asif Iqbal - 2 Year P.GDocument85 pagesMuscles of Mastication: - DR - Asif Iqbal - 2 Year P.GSaghar AbroNo ratings yet
- 2 - Enamel (Mahmoud Bakr)Document133 pages2 - Enamel (Mahmoud Bakr)MobarobberNo ratings yet
- An Overview of Removable Partial DentureDocument7 pagesAn Overview of Removable Partial DenturePatra PrimadanaNo ratings yet
- Department of Prosthodontics: By-Avantika Bohra Final YEARDocument37 pagesDepartment of Prosthodontics: By-Avantika Bohra Final YEARabhijeet100% (1)
- 03 Amelogenesis - EnglishDocument158 pages03 Amelogenesis - Englishvishal tiwaryNo ratings yet
- Local Anesthesia: O.R.Ganesh M.SC.D Endo University of The EastDocument71 pagesLocal Anesthesia: O.R.Ganesh M.SC.D Endo University of The EastDr.O.R.GANESAMURTHINo ratings yet
- Types of Balanced OcclusionDocument6 pagesTypes of Balanced Occlusionعلي صادق جعفرNo ratings yet
- Complications of Local AnesthesiaDocument24 pagesComplications of Local AnesthesiaAlexandroEscamillaNo ratings yet
- MCQ PaperDocument29 pagesMCQ PapermybdsexamsourceNo ratings yet
- SS 3rd Seminar Presentation - SALIVADocument104 pagesSS 3rd Seminar Presentation - SALIVAshwetaNo ratings yet
- Microsoft PowerPoint - Microbiology of Periodontal Disease (Compatibility Mode)Document20 pagesMicrosoft PowerPoint - Microbiology of Periodontal Disease (Compatibility Mode)Ahmed Tawfig Gamal100% (1)
- Muscle of Mastication: Presented By:-Dr. Shaifali Mdspg1 YearDocument72 pagesMuscle of Mastication: Presented By:-Dr. Shaifali Mdspg1 YearAtul GuptaNo ratings yet
- Review of Acrylic Removable Partial DenturesDocument64 pagesReview of Acrylic Removable Partial Denturesasop060% (1)
- Docslide - Us Dentogingival-UnitDocument53 pagesDocslide - Us Dentogingival-UnitarmNo ratings yet
- Dev of Hard & Soft PalateDocument94 pagesDev of Hard & Soft PalatepriyaNo ratings yet
- TMJ PDFDocument3 pagesTMJ PDFParneetNo ratings yet
- Pulp ProtactDocument7 pagesPulp ProtactFawaz AnwarNo ratings yet
- Neville's Atlas of Oral Pathology - TEXTODocument488 pagesNeville's Atlas of Oral Pathology - TEXTOgagandeep singh100% (1)
- Anatomy of PalateDocument33 pagesAnatomy of Palatekvellingiri0% (1)
- Local Anaesthesia and Minor Oral SurgeryDocument33 pagesLocal Anaesthesia and Minor Oral SurgeryAmina AbdullahiNo ratings yet
- 3 - Dentino-Pulp Complex (Mahmoud Bakr)Document129 pages3 - Dentino-Pulp Complex (Mahmoud Bakr)MobarobberNo ratings yet
- Local Anesthesia Part-1Document33 pagesLocal Anesthesia Part-1Abdul RazakNo ratings yet
- Fundamentals of Cavity PreparationDocument76 pagesFundamentals of Cavity Preparationragakodali0% (1)
- باثوو برزنتيشنDocument40 pagesباثوو برزنتيشنLojin HaddadNo ratings yet
- SEM 8 - Calcium HyrdroxideDocument130 pagesSEM 8 - Calcium HyrdroxideSwati NairNo ratings yet
- The PulpDocument58 pagesThe PulpkeerthanaNo ratings yet
- Amelogenesis: Prof. Shaleen ChandraDocument16 pagesAmelogenesis: Prof. Shaleen ChandraSheshayi RoyNo ratings yet
- Lec 16 Normal Radiographic AnatomyDocument56 pagesLec 16 Normal Radiographic Anatomyعباس اركان صيوان عطوانNo ratings yet
- TMJ and Muscles of MasticatoryDocument9 pagesTMJ and Muscles of MasticatoryFatima MartinezNo ratings yet
- Mandibular Movements Up L of DDocument79 pagesMandibular Movements Up L of DkrondanNo ratings yet
- DentinDocument88 pagesDentinSuhana Ahmed100% (1)
- Pharyngeal Arch Derivatives ChartDocument5 pagesPharyngeal Arch Derivatives Chartezaz000No ratings yet
- Oral Histology Quick ReviewDocument67 pagesOral Histology Quick ReviewTimothy Jairus LawNo ratings yet
- B - en AmelogenesisDocument23 pagesB - en Amelogenesisapi-371033150% (2)
- Assingment 2Document28 pagesAssingment 2nivitha naidu100% (1)
- 03 Connective TissueDocument60 pages03 Connective TissueMuhammad Khaled TaubehNo ratings yet
- Enamel: Click To Edit Master Subtitle StyleDocument106 pagesEnamel: Click To Edit Master Subtitle StyleManva MonishNo ratings yet
- Dentin and Its Clinical ConsiderationDocument97 pagesDentin and Its Clinical ConsiderationKrithikaNo ratings yet
- The MandibleDocument115 pagesThe MandiblenavjotsinghjassalNo ratings yet
- Fundamentals in Tooth Preparation: By-Pawar Hariom Jadhao SanjivaniDocument31 pagesFundamentals in Tooth Preparation: By-Pawar Hariom Jadhao SanjivaniMayuri DhanushwarNo ratings yet
- Fundamentals of Cavity Preparation MinDocument71 pagesFundamentals of Cavity Preparation MinA MINORNo ratings yet
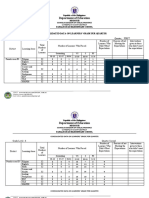
- Department of Education: Consolidated Data On Learners' Grade Per QuarterDocument4 pagesDepartment of Education: Consolidated Data On Learners' Grade Per QuarterUsagi HamadaNo ratings yet
- Aditya Academy Syllabus-II 2020Document7 pagesAditya Academy Syllabus-II 2020Tarun MajumdarNo ratings yet
- CE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Document6 pagesCE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Angelice Alliah De la CruzNo ratings yet
- Atomberg Gorilla FanDocument12 pagesAtomberg Gorilla FanjothamNo ratings yet
- File RecordsDocument161 pagesFile RecordsAtharva Thite100% (2)
- SAMPLE MCQuestions ByTopicsDocument45 pagesSAMPLE MCQuestions ByTopicsVeeru ManikantaNo ratings yet
- Banking Ombudsman 58Document4 pagesBanking Ombudsman 58Sahil GauravNo ratings yet
- Aristotle - OCR - AS Revision NotesDocument3 pagesAristotle - OCR - AS Revision NotesAmelia Dovelle0% (1)
- Executive Summary: 2013 Edelman Trust BarometerDocument12 pagesExecutive Summary: 2013 Edelman Trust BarometerEdelman100% (4)
- Waste Biorefinery Models Towards Sustainable Circular Bioeconomy Critical Review and Future Perspectives2016bioresource Technology PDFDocument11 pagesWaste Biorefinery Models Towards Sustainable Circular Bioeconomy Critical Review and Future Perspectives2016bioresource Technology PDFdatinov100% (1)
- SDS ERSA Rev 0Document156 pagesSDS ERSA Rev 0EdgarVelosoCastroNo ratings yet
- I. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)Document5 pagesI. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)thmeiz.17sNo ratings yet
- RH-A Catalog PDFDocument1 pageRH-A Catalog PDFAchmad KNo ratings yet
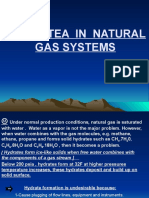
- Chapter 2 HydrateDocument38 pagesChapter 2 HydrateTaha Azab MouridNo ratings yet
- Raiders of SuluDocument1 pageRaiders of SuluBlexx LagrimasNo ratings yet
- Third Party Risk Management Solution - WebDocument16 pagesThird Party Risk Management Solution - Webpreenk8No ratings yet
- 12 Step Worksheet With QuestionsDocument26 pages12 Step Worksheet With QuestionsKristinDaigleNo ratings yet
- Designed For Severe ServiceDocument28 pagesDesigned For Severe ServiceAnthonyNo ratings yet
- Installation Instructions INI Luma Gen2Document21 pagesInstallation Instructions INI Luma Gen2John Kim CarandangNo ratings yet
- PDS DeltaV SimulateDocument9 pagesPDS DeltaV SimulateJesus JuarezNo ratings yet
- Arudha PDFDocument17 pagesArudha PDFRakesh Singh100% (1)
- Darkle Slideshow by SlidesgoDocument53 pagesDarkle Slideshow by SlidesgoADITI GUPTANo ratings yet
- ME-6501Computer Aided Design (CAD) WITH QB - BY Civildatas - Com 1Document85 pagesME-6501Computer Aided Design (CAD) WITH QB - BY Civildatas - Com 1Nathar ShaNo ratings yet
- Sony x300 ManualDocument8 pagesSony x300 ManualMarcosCanforaNo ratings yet
- Uniform Motion WorksheetDocument8 pagesUniform Motion Worksheetnikhil patro100% (1)
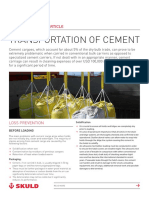
- Transportation of CementDocument13 pagesTransportation of CementKaustubh Joshi100% (1)
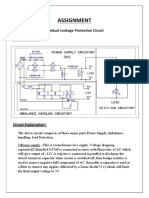
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDocument2 pagesAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNo ratings yet
- LC For Akij Biax Films Limited: CO2012102 0 December 22, 2020Document2 pagesLC For Akij Biax Films Limited: CO2012102 0 December 22, 2020Mahadi Hassan ShemulNo ratings yet
- Aashto M288-17 Product Selection GuideDocument1 pageAashto M288-17 Product Selection GuideDem DemNo ratings yet
- Multiple Choice Practice Questions For Online/Omr AITT-2020 Instrument MechanicDocument58 pagesMultiple Choice Practice Questions For Online/Omr AITT-2020 Instrument Mechanicمصطفى شاكر محمودNo ratings yet