You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- General Considerations Parasitology: Tropical DiseaseDocument5 pagesGeneral Considerations Parasitology: Tropical DiseaseAlliah SidicNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A.18 Hypochlorous-AcidDocument57 pagesA.18 Hypochlorous-AcidHervian LanangNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sleep DeprivationDocument8 pagesSleep DeprivationJona Riem NarvasaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Guidelines For Dental ServicesDocument6 pagesGuidelines For Dental Servicesdruzair007No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 1 - The Covid-19 Vaccine Is GENE THERAPY - David Martin BotW - Transcript - 01!11!2021Document7 pages1 - The Covid-19 Vaccine Is GENE THERAPY - David Martin BotW - Transcript - 01!11!2021bigbill138No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Lenz Medical ParasitologyDocument24 pagesLenz Medical ParasitologyArvin Delos SantosNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Rosenberg, Disease in HistoryDocument16 pagesRosenberg, Disease in Historyhector3nu3ezNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Bill GatesDocument180 pagesBill GatesRuth Candor100% (3)
- Lay LanguageDocument14 pagesLay LanguageOsama AldahamshehNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Health Care Services CBC NC IIDocument5 pagesHealth Care Services CBC NC IIcynthiaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- IFU Labnovation Ag Rapid Test - EnglishDocument2 pagesIFU Labnovation Ag Rapid Test - EnglisherlitaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Contoh Soal Uji Kompetensi Keperawatan KomunitasDocument39 pagesContoh Soal Uji Kompetensi Keperawatan KomunitasUmairohSetengahTiga67% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HepatitisDocument46 pagesHepatitisGusti Tirtha Drag JrNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Is-1479-Part-3.1977-Bacteriological Analysis of MilkDocument30 pagesIs-1479-Part-3.1977-Bacteriological Analysis of MilkStacy WilsonNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Test Bank For Basic Clinical Lab Competencies For Respiratory Care An Integrated Approach 5th Edition WhiteDocument9 pagesTest Bank For Basic Clinical Lab Competencies For Respiratory Care An Integrated Approach 5th Edition WhiteGeorge Rogers100% (41)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- SP Hic Manual PDFDocument76 pagesSP Hic Manual PDFANTO MATHINo ratings yet
- Mapeh Reviewer 3rd QuarterDocument3 pagesMapeh Reviewer 3rd QuarterIceyYamahaNo ratings yet
- Biomaterial-Based Antimicrobial Therapies For The Treatment of Bacterial InfectionsDocument16 pagesBiomaterial-Based Antimicrobial Therapies For The Treatment of Bacterial Infections徐勇No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- PolioDocument13 pagesPolioAhmadNo ratings yet
- Draft: The Principles of Infection Prevention and ControlDocument36 pagesDraft: The Principles of Infection Prevention and Controlandrel davidNo ratings yet
- MICP211 Midterm ReviewerDocument39 pagesMICP211 Midterm ReviewerKrista CruzNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- MT2 Group-3Document14 pagesMT2 Group-3Berdel PascoNo ratings yet
- Sepsis 3Document38 pagesSepsis 3EvanNo ratings yet
- PSM (Must Know)Document19 pagesPSM (Must Know)PranavNo ratings yet
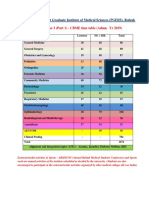
- 2019 CompetDocument64 pages2019 CompetKshirsagar DarshNo ratings yet
- Significance of History Taking Oral SurgeryDocument32 pagesSignificance of History Taking Oral SurgeryFourthMolar.com0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Surgical Site InfectionDocument35 pagesSurgical Site InfectionDetria Rahma GastiNo ratings yet
- Merrill Singer - The Anthropology of Infectious Disease (2014, Left Coast Press)Document321 pagesMerrill Singer - The Anthropology of Infectious Disease (2014, Left Coast Press)rina100% (1)
- 1BI0 1H Rms 20220224Document32 pages1BI0 1H Rms 20220224Musyoka DanteNo ratings yet
- NCP NewbornDocument21 pagesNCP NewbornGil Aswigui81% (27)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)