You might also like
- Concept 1 - Leadership & Management in NursingDocument652 pagesConcept 1 - Leadership & Management in Nursingezenz0205100% (3)
- NCM 105 Nursing Leadership and ManagementDocument295 pagesNCM 105 Nursing Leadership and ManagementMica Ann Dela Cruz100% (3)
- LEC 1 PRELIM Nursing Leadership and ManagementDocument307 pagesLEC 1 PRELIM Nursing Leadership and ManagementMae Montesena BreganzaNo ratings yet
- Task-Oriented Relationship-Oriented Participative Leadership Task-OrientedDocument17 pagesTask-Oriented Relationship-Oriented Participative Leadership Task-OrientedDENNIS N. MUÑOZNo ratings yet
- Nursing Leadership and ManagementDocument182 pagesNursing Leadership and ManagementAlain Dave90% (10)
- Nursing Leadership & ManagementDocument36 pagesNursing Leadership & ManagementPrince Paraiso100% (7)
- Nursing Leadership and ManagementDocument13 pagesNursing Leadership and ManagementChrisgr8100% (6)
- Nursing Leadership and Management Prelims Lesson 1-5Document4 pagesNursing Leadership and Management Prelims Lesson 1-5Paul Christian P. Santos, RN100% (14)
- Nursing Leadership and ManagementDocument8 pagesNursing Leadership and Managementaurezea50% (2)
- Unit 1 Chapter 2 Nursing Leadership and ManagementDocument9 pagesUnit 1 Chapter 2 Nursing Leadership and Managementfree_books_jym100% (1)
- Nursing Management 2Document118 pagesNursing Management 2Jasmin Jacob100% (36)
- Nursing Leadership and Management PDFDocument10 pagesNursing Leadership and Management PDFhahahahaaaaaaa100% (9)
- Nursing Leadership and ManagementDocument43 pagesNursing Leadership and Managementbajaoc95% (22)
- Leadership and ManagementDocument216 pagesLeadership and ManagementYum C75% (4)
- Nursing Leadership and Management ExamsDocument4 pagesNursing Leadership and Management ExamsMarisol Jane Jomaya67% (9)
- Nursing Leadership and ManagementDocument48 pagesNursing Leadership and ManagementDarl DacdacNo ratings yet
- Nursing Leadership - Reviewquestion 1Document6 pagesNursing Leadership - Reviewquestion 1Darren Jay Nikazy80% (5)
- Nursing Management & LeadershipDocument8 pagesNursing Management & LeadershipDjhoanna Kriska88% (42)
- Nursing ManagementDocument24 pagesNursing ManagementSimran Josan100% (1)
- NURSING Management ProcessDocument80 pagesNURSING Management Processma_tabora628391% (33)
- Nursing Management LeadershipDocument8 pagesNursing Management LeadershipIvy Balza Caber100% (1)
- Nursing Leadership TheoriesDocument121 pagesNursing Leadership TheoriesHoneylet Villanueva67% (3)
- Nursing Leadership and ManagementDocument3 pagesNursing Leadership and ManagementRI NA100% (1)
- Controlling in Nursing ManagementDocument45 pagesControlling in Nursing Managementverna92% (37)
- NLM QuestionsDocument15 pagesNLM Questionsleoboi_leoboi81% (16)
- Nursing Management Process and FunctionsDocument151 pagesNursing Management Process and FunctionsJaq Kyatchon90% (29)
- Leadership and Management in NursingDocument5 pagesLeadership and Management in NursingSolsona Natl HS Maananteng100% (1)
- Nursing Management - Concepts and Principles of ManagementDocument4 pagesNursing Management - Concepts and Principles of Managementsoundaramilangovan254989% (9)
- Directing in Nursing ManagementDocument27 pagesDirecting in Nursing Managementwersken100% (4)
- The Organizational Structure of Nursing Service DepartmentDocument5 pagesThe Organizational Structure of Nursing Service DepartmentNikki Arra100% (8)
- Leadership and ManagementDocument24 pagesLeadership and Managementansh2195100% (2)
- Lec Note - NSG Leadership and ManagementDocument86 pagesLec Note - NSG Leadership and Managementederlyn21No ratings yet
- CBQ - Leadership and Management in Nursing 2009Document14 pagesCBQ - Leadership and Management in Nursing 2009Lizette Leah Ching95% (20)
- Nursing Leadership NCM 105: Madeline N. Gerzon, RN, MM Clinical InstructorDocument74 pagesNursing Leadership NCM 105: Madeline N. Gerzon, RN, MM Clinical Instructormgerzon93% (15)
- Nursing Leadership and Management Practice TestDocument6 pagesNursing Leadership and Management Practice TestHaifi Hun0% (1)
- ControllingDocument8 pagesControllingAnjo Pasiolco Canicosa100% (2)
- Nursing AdministrationDocument71 pagesNursing AdministrationJoYCe100% (5)
- Organizing Management NursingDocument31 pagesOrganizing Management NursingAlfitoHarfahGiffary100% (1)
- Leadership in NursingDocument31 pagesLeadership in NursingMichael Urrutia100% (1)
- Leadership and Managementfinal Nursing ReviewerDocument23 pagesLeadership and Managementfinal Nursing ReviewerPhilip Simangan100% (5)
- DelegationDocument58 pagesDelegationkrishnasree100% (1)
- Nursing Management IntroductionDocument42 pagesNursing Management Introductionanreilegarde100% (5)
- Midterm Leadership and Management (MCN 107) EXAMDocument26 pagesMidterm Leadership and Management (MCN 107) EXAMsophi30100% (1)
- LMR Notes 1Document15 pagesLMR Notes 1Krisly Jade TeoNo ratings yet
- Educational LeadershipDocument46 pagesEducational LeadershipNiño Angelo AustriaNo ratings yet
- Being An Effective LeaderDocument19 pagesBeing An Effective LeaderHamza AliNo ratings yet
- LeadershipDocument53 pagesLeadershipcute_little4596% (72)
- Leadership and ManagementDocument5 pagesLeadership and ManagementYmon TuallaNo ratings yet
- What Is Your Personaldefinition of Leadership? Definition of LeadershipDocument11 pagesWhat Is Your Personaldefinition of Leadership? Definition of LeadershipAnnaMae MalapitNo ratings yet
- Leadershi P: Group 4 - Nazareno, Jhonsin E. - Tudon, Sittie Raiza Bantas - Sali, Alta-Abbon Mamako - Ibrahim, Madani GDocument28 pagesLeadershi P: Group 4 - Nazareno, Jhonsin E. - Tudon, Sittie Raiza Bantas - Sali, Alta-Abbon Mamako - Ibrahim, Madani GHazel Mae JumaaniNo ratings yet
- Hbo Chapter 8 - LeadershipDocument72 pagesHbo Chapter 8 - LeadershipAbegail Perez100% (1)
- LeadingDocument6 pagesLeadingdummyNo ratings yet
- Em 502 LeadershipDocument4 pagesEm 502 LeadershipAngelie CayananNo ratings yet
- Leadership & ManagementDocument83 pagesLeadership & ManagementJasmin Jacob92% (13)
- Leadership & Influence ProcessDocument43 pagesLeadership & Influence ProcessAnnalene de guzmanNo ratings yet
- LeadershipDocument6 pagesLeadershipayubwasongaNo ratings yet
- Hbo Chapter 8 ReportDocument72 pagesHbo Chapter 8 ReportAbegail PerezNo ratings yet
- LeadershipDocument2 pagesLeadershipNeha KanojiyaNo ratings yet
- Leadership: Leadership Is The Ability To Influence A Group Toward The Achievement of A Vision or Set of GoalsDocument5 pagesLeadership: Leadership Is The Ability To Influence A Group Toward The Achievement of A Vision or Set of GoalsSadia RasoolNo ratings yet
- (Front and Back Page) It 23 ProjectDocument2 pages(Front and Back Page) It 23 Projectpaul andrew laranjo asuncionNo ratings yet
- Mathematics CoverDocument3 pagesMathematics Coverpaul andrew laranjo asuncionNo ratings yet
- DiabetesDocument2 pagesDiabetespaul andrew laranjo asuncionNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologypaul andrew laranjo asuncionNo ratings yet
- Front Page.Document1 pageFront Page.paul andrew laranjo asuncionNo ratings yet
- Nursing ManagementDocument38 pagesNursing Managementpaul andrew laranjo asuncion100% (1)
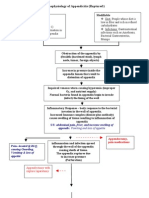
- Pathophysiology of Appendicitis (Ruptured)Document2 pagesPathophysiology of Appendicitis (Ruptured)paul andrew laranjo asuncion100% (2)
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Corr Leadership and Management of McDonaldDocument14 pagesCorr Leadership and Management of McDonaldSly Bee ShittuNo ratings yet
- CFLM 2 HandoutsDocument9 pagesCFLM 2 HandoutsBcfi CriminologyNo ratings yet
- The Art and Science of Leadership 6e Afsaneh Nahavandi Test BankDocument5 pagesThe Art and Science of Leadership 6e Afsaneh Nahavandi Test BankIvan Olegov0% (2)
- (22560173 - Economics and Culture) Ethical Leadership - Meaning and Measurement. Latvian Retail Traders' PerspectiveDocument8 pages(22560173 - Economics and Culture) Ethical Leadership - Meaning and Measurement. Latvian Retail Traders' PerspectiveGosa GutaNo ratings yet
- Black LeadershipDocument22 pagesBlack LeadershipHillary Dwainee R. LorenzoNo ratings yet
- Transformational Leadership Theory - Meaning, Criticisms and Its ImplicationsDocument1 pageTransformational Leadership Theory - Meaning, Criticisms and Its ImplicationsSatyam SachanNo ratings yet
- Leadership Styles and Employee Satisfaction A CorrDocument14 pagesLeadership Styles and Employee Satisfaction A CorrJarupla DeepakNo ratings yet
- Organizational BehaviourDocument43 pagesOrganizational BehaviourAndree JaiswalNo ratings yet
- Effects of Leadership Styles On Job Sati PDFDocument10 pagesEffects of Leadership Styles On Job Sati PDFJisha ShajiNo ratings yet
- Leadership Styles in MalaysiaDocument245 pagesLeadership Styles in MalaysiaJynn Yeow69% (13)
- Leadership AssignmentDocument9 pagesLeadership AssignmentKevin JacksonNo ratings yet
- Leadership and Performance Beyond Expectations: Click HereDocument6 pagesLeadership and Performance Beyond Expectations: Click HereParas Pathar0% (1)
- Penerapan Gaya Kepemimpinan Transformasional Dalam Manajemen PAUD Di Kecamatan Sidorejo SalatigaDocument13 pagesPenerapan Gaya Kepemimpinan Transformasional Dalam Manajemen PAUD Di Kecamatan Sidorejo SalatigaRikiRikjanUvNo ratings yet
- LeadershipStyle BEPAMDocument20 pagesLeadershipStyle BEPAMJowana Abou shakraNo ratings yet
- 10 1108 - Jocm 02 2021 0045Document31 pages10 1108 - Jocm 02 2021 0045Solihin SolihinNo ratings yet
- Leader 3Document65 pagesLeader 3Aklilu100% (1)
- 4160 Chapter 12 QuizzesDocument43 pages4160 Chapter 12 QuizzesCoriana SurellsNo ratings yet
- Chapter One: 1.1. Back Ground of The StudyDocument65 pagesChapter One: 1.1. Back Ground of The Studymubarek oumerNo ratings yet
- Yiheyis Final PDFDocument53 pagesYiheyis Final PDFMuluken AlemuNo ratings yet
- School Leadership and Resource MobilizationDocument83 pagesSchool Leadership and Resource Mobilizationalemu tessemaNo ratings yet
- Effective Communcation 2Document12 pagesEffective Communcation 2nehagomale26No ratings yet
- Leadership Style and PhilosophyDocument5 pagesLeadership Style and Philosophyapi-558221200No ratings yet
- Sample Outline Imrad 1Document18 pagesSample Outline Imrad 1JULIETO TANNo ratings yet
- Leaders RoleDocument37 pagesLeaders RoleSelamu Yisihak Handiso 韩士兰 (Ph.D., Researcher and Robot R & D engineer)No ratings yet
- Perceptions of Leadership - Impact of Leadership Style and Gender - 2Document110 pagesPerceptions of Leadership - Impact of Leadership Style and Gender - 2Vũ HườngNo ratings yet
- The Relationship of Adversity Quotient and LeadershipDocument29 pagesThe Relationship of Adversity Quotient and LeadershipLicia SalimNo ratings yet
- Module 2 - HUT 310 - Ktunotes - inDocument157 pagesModule 2 - HUT 310 - Ktunotes - inNeerajNo ratings yet
- Reflection On Leadership and Followership StyleDocument6 pagesReflection On Leadership and Followership Styleapi-283071924No ratings yet
- Assessing Leadership Styles and Organisational Context Dulewicz and HiggsDocument19 pagesAssessing Leadership Styles and Organisational Context Dulewicz and HiggsHaithem Darwich0% (1)
- Yoseph MogesDocument86 pagesYoseph Mogesnatud6No ratings yet