You might also like
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Chapter 45 CanvasDocument49 pagesChapter 45 CanvasSheNo ratings yet
- Reviewer Skeletal To EndoDocument46 pagesReviewer Skeletal To EndoSophia CaisipNo ratings yet
- 1.introduction To AnatomyDocument30 pages1.introduction To AnatomyDixonLing100% (1)
- Hearing and EquilibriumDocument30 pagesHearing and EquilibriumabdirizakNo ratings yet
- Special Senses EYEDocument27 pagesSpecial Senses EYENadiabloshii NadiabloshiiNo ratings yet
- An Organ That Receives and Relays Information About The Body's Senses To The BrainDocument59 pagesAn Organ That Receives and Relays Information About The Body's Senses To The BrainIsarra AmsaluNo ratings yet
- Orthopedic Devices DDocument31 pagesOrthopedic Devices Dmakenawairimu30No ratings yet
- Musculo Care Modalities 2 PDFDocument44 pagesMusculo Care Modalities 2 PDFAhmad FaujiNo ratings yet
- Endocrine System Reviewer - BAYLONDocument6 pagesEndocrine System Reviewer - BAYLONElijah Joaquin Payumo BaylonNo ratings yet
- Nutritional Guidelines For FilipinosDocument4 pagesNutritional Guidelines For FilipinosMademoiselle Kayetty67% (3)
- Cardiovascular System: More Than Just The HeartDocument34 pagesCardiovascular System: More Than Just The HearteliseudesafateNo ratings yet
- Hygiene Funda 1 2nd SemDocument22 pagesHygiene Funda 1 2nd Semlegion alexandersNo ratings yet
- Pretest FinalDocument2 pagesPretest FinalMatthew Pina0% (1)
- Digestive SystemDocument41 pagesDigestive SystemRotsen B. VelascoNo ratings yet
- Partograph: (Use This Form For Monitoring Active Labour)Document1 pagePartograph: (Use This Form For Monitoring Active Labour)Omar Khalif Amad PendatunNo ratings yet
- BloodDocument197 pagesBloodNimesh Sharma100% (1)
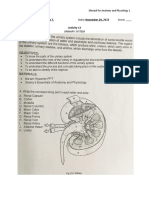
- Urinary SystemDocument5 pagesUrinary SystemJushelle Anne Tigoy Pilare100% (1)
- Chapter 8 - The VitaminsDocument3 pagesChapter 8 - The VitaminsYcell Latido100% (1)
- Anatomy Unit 7 - Physiology of The Skeletal SystemDocument22 pagesAnatomy Unit 7 - Physiology of The Skeletal SystemRi Chard100% (1)
- HPPDocument28 pagesHPPVfinNo ratings yet
- Anatomy and Physiology Lecture - Midterm (Labelling)Document15 pagesAnatomy and Physiology Lecture - Midterm (Labelling)KRISTINE ZAINAB PUENTE100% (1)
- Endocrine SystemDocument4 pagesEndocrine SystemMary Louwelyn GurreaNo ratings yet
- Lymph SystemDocument7 pagesLymph SystemghaiathNo ratings yet
- Fertilization and Fetal Development Abd CirculiationDocument54 pagesFertilization and Fetal Development Abd CirculiationMohnnad Hmood AlgaraybhNo ratings yet
- Assessing AbdomenDocument33 pagesAssessing Abdomenjaypee01No ratings yet
- Sensory Physiology Student ProtocolDocument18 pagesSensory Physiology Student ProtocolManuel Alejandro Chiguay GonzalezNo ratings yet
- AssessmentDocument65 pagesAssessmentRitaNo ratings yet
- Assessing The AbdomenDocument18 pagesAssessing The Abdomenmartinezrose32No ratings yet
- Musculoskeletal Anatomy and Physiology 5Document36 pagesMusculoskeletal Anatomy and Physiology 5Dennis Nabor Muñoz, RN,RMNo ratings yet
- Circulatory System FrogDocument9 pagesCirculatory System FrogLeticiaNo ratings yet
- D.5. Oxygenation and PerfusionDocument98 pagesD.5. Oxygenation and PerfusionTricia Denise EstabilloNo ratings yet
- BSC Biotechnology Syllabus Mqps 06112017Document38 pagesBSC Biotechnology Syllabus Mqps 06112017rupaNo ratings yet
- Welcome To The Control System of The BodyDocument31 pagesWelcome To The Control System of The BodypadiosNo ratings yet
- Please Perform A Upper Limb MOTOR Neurological Examination. After 5 Minutes I Will Ask You Some QuestionsDocument2 pagesPlease Perform A Upper Limb MOTOR Neurological Examination. After 5 Minutes I Will Ask You Some QuestionsMu AbNo ratings yet
- M M M M: By: Jan Michael Khalid L. MacarambonDocument23 pagesM M M M: By: Jan Michael Khalid L. Macarambonxtaticboy82No ratings yet
- Guide To History TakingDocument55 pagesGuide To History TakingGabriella Hild100% (1)
- Taenias IsDocument56 pagesTaenias Iseliwaja100% (1)
- Reading Food Labels LPDocument11 pagesReading Food Labels LPapi-272272803No ratings yet
- Anatomy of Male Reproductive OrgansDocument18 pagesAnatomy of Male Reproductive OrgansPutri HolmesNo ratings yet
- Accessory OrgansDocument18 pagesAccessory OrgansDaniel AtiehNo ratings yet
- Chapter 8: Nervous SystemDocument15 pagesChapter 8: Nervous SystemAndrea BoocNo ratings yet
- Laboratory ActivityDocument15 pagesLaboratory ActivityChippy RabeNo ratings yet
- Surgical IncisionDocument35 pagesSurgical IncisionJoshua SmithNo ratings yet
- Fluids and Electrolytes-2Document82 pagesFluids and Electrolytes-2Jem Loterte100% (1)
- Female and Male GenitaliaDocument5 pagesFemale and Male GenitaliaMary Mae BuellaNo ratings yet
- Maintaining The New Partogram: Prepared By: KMIU Ranasinghe & HKDK NadeeshaniDocument27 pagesMaintaining The New Partogram: Prepared By: KMIU Ranasinghe & HKDK Nadeeshanifei cuaNo ratings yet
- Partograf Versi Lengkap Dari Jaman Fase Laten Sampe Modified InggrisDocument101 pagesPartograf Versi Lengkap Dari Jaman Fase Laten Sampe Modified InggrispolygoneNo ratings yet
- 2 Lecture CardioDocument46 pages2 Lecture Cardiodr_mohanad100% (1)
- Anatomy PHysiologyDocument43 pagesAnatomy PHysiologyJoyce Hannah ReytanaNo ratings yet
- Normal NewbornAssessmentDocument53 pagesNormal NewbornAssessmentMidori SanNo ratings yet
- Anatomy of The BreastDocument6 pagesAnatomy of The BreastJuliana Andres100% (1)
- Bricsinnursingeducation PDFDocument6 pagesBricsinnursingeducation PDFshaikNo ratings yet
- Body TissuesDocument29 pagesBody TissuesPurplesmilezNo ratings yet
- 1 Bony PelvisDocument50 pages1 Bony PelvisNicole NgoNo ratings yet
- Heart Failure in ChildhoodDocument43 pagesHeart Failure in Childhoodhusnajihah18No ratings yet
- 2.2.2.A FoodLabelsFDocument5 pages2.2.2.A FoodLabelsFMarjaan KhanNo ratings yet
- Cardiovascular System: K. Hariharan Iv Eee - 'B'Document33 pagesCardiovascular System: K. Hariharan Iv Eee - 'B'Hari Haran100% (1)
- Breech Presentation 1Document33 pagesBreech Presentation 1Cristina StanleeNo ratings yet
- Basic ECGDocument19 pagesBasic ECGQuolette Constante100% (1)
- Leadership and ManagementDocument116 pagesLeadership and ManagementQuolette ConstanteNo ratings yet
- High Risk Pregnancy FinaleDocument149 pagesHigh Risk Pregnancy FinaleQuolette Constante100% (1)
- Management and Theorists 001Document75 pagesManagement and Theorists 001Quolette Constante100% (3)
- PlanningDocument96 pagesPlanningQuolette ConstanteNo ratings yet
- ECG Power PointDocument33 pagesECG Power PointQuolette ConstanteNo ratings yet
- Intentional Wrongs: - Intentional Tortuous Acts That Arise in The Performance of DutiesDocument34 pagesIntentional Wrongs: - Intentional Tortuous Acts That Arise in The Performance of DutiesQuolette ConstanteNo ratings yet
- Airway Obstruction and Foreign BodiesDocument26 pagesAirway Obstruction and Foreign BodiesQuolette ConstanteNo ratings yet
- 17 AntibioticsDocument67 pages17 AntibioticsQuolette ConstanteNo ratings yet
- Employee Selection & PlacementDocument51 pagesEmployee Selection & PlacementQuolette ConstanteNo ratings yet
- Nursing Leadership and ManagementDocument305 pagesNursing Leadership and Managementpaul andrew laranjo asuncion97% (29)
- Medical Surgical Nursing BulletsDocument143 pagesMedical Surgical Nursing BulletsJennye100% (3)
- 18 Antivirals UpdDocument19 pages18 Antivirals Updakazukin002100% (4)
- Disaster FinalDocument260 pagesDisaster FinalQuolette ConstanteNo ratings yet
- Handout PrenatalDocument5 pagesHandout PrenatalCiella Dela Cruz100% (2)
- Respiratory SystemDocument192 pagesRespiratory SystemQuolette Constante100% (1)
- Neuro DisordersDocument159 pagesNeuro DisordersQuolette Constante100% (1)
- Case Study Ugib Lower MBDocument65 pagesCase Study Ugib Lower MBQuolette Constante100% (1)
- Geriatric NursingDocument46 pagesGeriatric NursingQuolette Constante100% (2)
- Disturbance in Perception & Coordination: Mr. Carlo S. HidalgoDocument149 pagesDisturbance in Perception & Coordination: Mr. Carlo S. HidalgoYsn FabonNo ratings yet
- 04 Cholinergic Blockers UpdDocument58 pages04 Cholinergic Blockers Updakazukin002100% (1)
- Health and Illness KoDocument57 pagesHealth and Illness KoQuolette ConstanteNo ratings yet
- CNS DepressantsDocument27 pagesCNS DepressantsCodered ReviewNo ratings yet
- Health and IllnessDocument125 pagesHealth and IllnessQuolette ConstanteNo ratings yet
- Dosage & Solutions Intake & OutputDocument166 pagesDosage & Solutions Intake & OutputQuolette ConstanteNo ratings yet
- PainDocument59 pagesPainQuolette ConstanteNo ratings yet
- Genito Urinary InjuriesDocument73 pagesGenito Urinary InjuriesQuolette ConstanteNo ratings yet
- Genitp Urinary SystemDocument200 pagesGenitp Urinary SystemQuolette ConstanteNo ratings yet
- Loss, Grieving & DeathDocument59 pagesLoss, Grieving & DeathQuolette ConstanteNo ratings yet
- 2014 CONTINUUM Neurologic Complications of Rheumatic DiseaseDocument13 pages2014 CONTINUUM Neurologic Complications of Rheumatic DiseaseKarl Jimenez SeparaNo ratings yet
- Tiki Taka CK RheumatologyDocument15 pagesTiki Taka CK RheumatologykeyurbNo ratings yet
- 50 92 1 SM PDFDocument9 pages50 92 1 SM PDFWahyuni S FitriNo ratings yet
- MCQ in MedicineDocument18 pagesMCQ in MedicineEslamAlmassri75% (4)
- Development and Evaluation of Novel DDS For Topical Delivery of Quercetin For Treatment of Rheumatoid ArthritisDocument16 pagesDevelopment and Evaluation of Novel DDS For Topical Delivery of Quercetin For Treatment of Rheumatoid ArthritisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rheumatoid Arthritis DrugsDocument7 pagesRheumatoid Arthritis DrugsSANKET ROUTNo ratings yet
- IVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesDocument151 pagesIVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesMarc Imhotep Cray, M.D.100% (2)
- Rheumatoid ArthritisDocument28 pagesRheumatoid ArthritisNisya Andesita HNo ratings yet
- NSAIDSDocument19 pagesNSAIDSDonna Kelly DuranNo ratings yet
- Clinical Case JiaDocument28 pagesClinical Case JiaShymaNo ratings yet
- The Arthritis Diet Supplementation Plan - DR AxeDocument5 pagesThe Arthritis Diet Supplementation Plan - DR AxeSu H HarthyNo ratings yet
- Neumann: Kinesiology of The Musculoskeletal System, 2nd EditionDocument4 pagesNeumann: Kinesiology of The Musculoskeletal System, 2nd EditionVictor MarianNo ratings yet
- Problem Solving in RheumatologyDocument293 pagesProblem Solving in RheumatologyGaudeamus IgiturNo ratings yet
- IDECDocument33 pagesIDECcmlimNo ratings yet
- CS236 Homework Help 3Document4 pagesCS236 Homework Help 3Akun mobile LegendNo ratings yet
- Medicines List & Margin - PPDocument23 pagesMedicines List & Margin - PPKrishna SinghNo ratings yet
- Management of Rheumatoid Arthritis 2019Document76 pagesManagement of Rheumatoid Arthritis 2019Wila Gatchalian67% (3)
- RA1Document19 pagesRA1Ioana Omnia OkamNo ratings yet
- Rheumatoid Arthritis OsteoarthritisDocument33 pagesRheumatoid Arthritis OsteoarthritisTri Hastuti HendrayaniNo ratings yet
- Artikel Bahasa Inggris Tentang Kesehatan IDocument3 pagesArtikel Bahasa Inggris Tentang Kesehatan IRestu Yogi Fahlevi100% (2)
- Dr. Rachmat Gunadi - Vitamin D - Autoimmune Prodia Final PDFDocument38 pagesDr. Rachmat Gunadi - Vitamin D - Autoimmune Prodia Final PDFNururrohmahNo ratings yet
- Autoimmune DiseasesDocument14 pagesAutoimmune Diseasesdr_swaralipiNo ratings yet
- Immunology 2Document69 pagesImmunology 2pikachuNo ratings yet
- High Prevalence of Potential Drug-Drug Interactions For Psoriasis Patients Prescribed Methotrexate or Cyclosporine For Psoriasis: Associated Clinical and Economic Outcomes in Real-World PracticeDocument10 pagesHigh Prevalence of Potential Drug-Drug Interactions For Psoriasis Patients Prescribed Methotrexate or Cyclosporine For Psoriasis: Associated Clinical and Economic Outcomes in Real-World PracticeshaniNo ratings yet
- Nutrition Interventions in Rheumatoid ArDocument11 pagesNutrition Interventions in Rheumatoid ArJULIETANo ratings yet
- Arthritis PPT For ClassDocument62 pagesArthritis PPT For ClassMayank Sarie100% (3)
- Rheumatoid Arthritis PDFDocument44 pagesRheumatoid Arthritis PDFnahmae oedNo ratings yet
- Glenmark Analyst PPTDocument90 pagesGlenmark Analyst PPTMahesh NaikNo ratings yet
- Pharmaceutical Analytical ChemistryDocument5 pagesPharmaceutical Analytical ChemistryGeorge MoshiashviliNo ratings yet