You might also like
- Polymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandPolymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (2)
- Polymyalgia RheumaticaDocument27 pagesPolymyalgia RheumaticaBima Anugrah KusumaNo ratings yet
- Lecture INST-100294 2023 12 08 22 26 10Document62 pagesLecture INST-100294 2023 12 08 22 26 10Pughal PrabakarNo ratings yet
- Chap 321: GideonjcaballesDocument73 pagesChap 321: GideonjcaballesMichelle ThereseNo ratings yet
- Final Rheumatoid ArthritisDocument27 pagesFinal Rheumatoid ArthritisAmmarNo ratings yet
- Kuliah Path Clin MSK 2017Document26 pagesKuliah Path Clin MSK 2017LioraNo ratings yet
- Ra Sle MSDocument60 pagesRa Sle MSDionisius KevinNo ratings yet
- Morning Report: Presented by Christopher El Hadi Moderated by Dr. Colette HannaDocument31 pagesMorning Report: Presented by Christopher El Hadi Moderated by Dr. Colette Hannabtp7b7gmggNo ratings yet
- CP - Acute Onset ParaparesisDocument47 pagesCP - Acute Onset ParaparesisParag DashatwarNo ratings yet
- Final Rheumatoid Arthritis - PPT 2Document51 pagesFinal Rheumatoid Arthritis - PPT 2Tino kashiriNo ratings yet
- Overview of Rheumatoid Arthritis: Naureen Mirza, MD May 10, 2010Document34 pagesOverview of Rheumatoid Arthritis: Naureen Mirza, MD May 10, 2010csingleton2364No ratings yet
- Joint Pain Case StudiesDocument51 pagesJoint Pain Case StudiesNaziBrola TsivadzeNo ratings yet
- VASCULITISDocument79 pagesVASCULITISSol CamusNo ratings yet
- Systemic Lupus Erythematosus and Neuropsychiatric DiseaseDocument56 pagesSystemic Lupus Erythematosus and Neuropsychiatric DiseaseHerry HendrayadiNo ratings yet
- Final Rheumatoid ArthritisDocument58 pagesFinal Rheumatoid ArthritisShivalingaiah GirishNo ratings yet
- Vasculopathies - Spring 2011Document35 pagesVasculopathies - Spring 2011uwpacmanNo ratings yet
- Takayasu ArteritisDocument53 pagesTakayasu ArteritisSuruchi Jagdish Sharma50% (2)
- Morning Report: Aaron Mccoy, MD, Pgy3Document16 pagesMorning Report: Aaron Mccoy, MD, Pgy3Emily EresumaNo ratings yet
- Pembahasan To Online 3Document201 pagesPembahasan To Online 3Fate DreamworkNo ratings yet
- Ankylosing Spondylitis Early Diagnosis & Pitfall - University of Colorado Health and Science CenterDocument17 pagesAnkylosing Spondylitis Early Diagnosis & Pitfall - University of Colorado Health and Science CenterChictopia SweetNo ratings yet
- Polymyalgia Rheumatica: Sarah Hughes, MD Morning Report January 24, 2006Document22 pagesPolymyalgia Rheumatica: Sarah Hughes, MD Morning Report January 24, 2006AbigaleNo ratings yet
- UWorld JournalDocument21 pagesUWorld JournalMaria SvarkaNo ratings yet
- Systemic Onset JIADocument11 pagesSystemic Onset JIAEmily EresumaNo ratings yet
- Juvenile DermatomyositisDocument22 pagesJuvenile DermatomyositisEmily EresumaNo ratings yet
- Rheumatology MRCP1Document186 pagesRheumatology MRCP1Raouf Ra'fat Soliman100% (3)
- Vasculitis Syndrome (VS) : Dr. Julius Roma, SP ADocument45 pagesVasculitis Syndrome (VS) : Dr. Julius Roma, SP ADavid ChristianNo ratings yet
- ArthritisDocument56 pagesArthritisyulitamustikasariNo ratings yet
- Last Look Nephrology & Rheumatology (Medicine Must Know)Document43 pagesLast Look Nephrology & Rheumatology (Medicine Must Know)rohankananiNo ratings yet
- Acute Rheumatic FeverDocument37 pagesAcute Rheumatic FeverQadriyah Ramadhani100% (1)
- ARTHRITIS-by Ayesigwa GeraldDocument38 pagesARTHRITIS-by Ayesigwa GeraldAyesigwa Gerald96No ratings yet
- Rheumatic Fever: Prof. A K M MohibullahDocument42 pagesRheumatic Fever: Prof. A K M MohibullahNavojit ChowdhuryNo ratings yet
- Oncologic EmergenciesDocument163 pagesOncologic EmergenciesGeorge BoaduNo ratings yet
- Approach To Rheum PTDocument44 pagesApproach To Rheum PTjiojimalaniNo ratings yet
- Avascular Necrosis of Femoral HeadDocument50 pagesAvascular Necrosis of Femoral HeadStar CruiseNo ratings yet
- Polymyalgia Rheumatica: Dr. Monalisa, SPPDDocument23 pagesPolymyalgia Rheumatica: Dr. Monalisa, SPPDPutri Sari SeptirianiNo ratings yet
- Spektrum AIDocument55 pagesSpektrum AIOgizWaraNo ratings yet
- Interstitial Lung Disease in Anti-Synthetase SyndromeDocument4 pagesInterstitial Lung Disease in Anti-Synthetase SyndromeT. SimopoulouNo ratings yet
- Mixed Connective Tissue Disease That WasDocument10 pagesMixed Connective Tissue Disease That Wassaideh naghibiNo ratings yet
- Reumato and EndocrineDocument106 pagesReumato and Endocrinehasanatiya41No ratings yet
- Rheumatic Fever & Rheumatic Heart DiseaseDocument87 pagesRheumatic Fever & Rheumatic Heart DiseaseMarianoNo ratings yet
- Systemic Lupus Erythematosus: Supervisor: Dr. Dr. Faridin HP, SP - PD-KR Radina Thahir Nurul ArifahDocument34 pagesSystemic Lupus Erythematosus: Supervisor: Dr. Dr. Faridin HP, SP - PD-KR Radina Thahir Nurul ArifahRadina Bi RanNo ratings yet
- Cerebral ToxoplasmosisDocument57 pagesCerebral Toxoplasmosismarie gold sorilaNo ratings yet
- Autoimmune Disorders of Central Nervous System: Lutsenko I.LDocument46 pagesAutoimmune Disorders of Central Nervous System: Lutsenko I.LDrhikmatullah SheraniNo ratings yet
- Diagnosisfor PEDocument28 pagesDiagnosisfor PEMohd Syaiful Mohd ArisNo ratings yet
- 0009 Rheumatology Notes 2015 PDFDocument56 pages0009 Rheumatology Notes 2015 PDFMuhammad HaneefNo ratings yet
- Rheumatology For AMK: Abhinav Singh PMSDocument43 pagesRheumatology For AMK: Abhinav Singh PMSTerrence ChanNo ratings yet
- Morning Report: Jawaria K. Alam, MD/PGY3Document20 pagesMorning Report: Jawaria K. Alam, MD/PGY3Emily EresumaNo ratings yet
- Systemic Lupus ErythematosusDocument3 pagesSystemic Lupus ErythematosusAlya Putri KhairaniNo ratings yet
- ANCA Associated VasculitisDocument62 pagesANCA Associated VasculitispoluashokNo ratings yet
- Enfermedades LisosomalesDocument32 pagesEnfermedades LisosomalesJonathanOmarLaraAcevedoNo ratings yet
- Polimialgia RematikaDocument23 pagesPolimialgia RematikaArtika MayandaNo ratings yet
- Rheumatoid ArthritisDocument37 pagesRheumatoid ArthritisPetit NacarioNo ratings yet
- Rheumatic FeverDocument87 pagesRheumatic FeverFarida Mawaddah Husna100% (1)
- Approach To ARTHRITISDocument46 pagesApproach To ARTHRITISkalfNo ratings yet
- CPD MSK19-Thu-1-SchwabDocument51 pagesCPD MSK19-Thu-1-SchwabGiaNo ratings yet
- Acute Pulmonary Embolism Final YearDocument52 pagesAcute Pulmonary Embolism Final YearUzma BanoNo ratings yet
- Histiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesDocument41 pagesHistiocytic Disorders Diagnosis and Treatment: Resident Education Lecture SeriesChetan SekhriNo ratings yet
- Fever of Unknown Origin (FUO)Document55 pagesFever of Unknown Origin (FUO)mohamed hanyNo ratings yet
- Arterial ThrombosisrheumroundsDocument49 pagesArterial ThrombosisrheumroundsBiniyam AsratNo ratings yet
- Plab! 2Document8 pagesPlab! 2shafiqullah IbrahimiNo ratings yet
- Cinderella: From The Blue Fairy Book of Andrew LangDocument7 pagesCinderella: From The Blue Fairy Book of Andrew LangnizamianNo ratings yet
- 3rd Sunday After TrinityDocument11 pages3rd Sunday After TrinityHmkEnochNo ratings yet
- John 20 Study GuideDocument11 pagesJohn 20 Study GuideCongregation Shema YisraelNo ratings yet
- HistogramDocument7 pagesHistogramTesfaye MinaleNo ratings yet
- Making Effective Pres. Academic Lit I. Weeks 4 5Document27 pagesMaking Effective Pres. Academic Lit I. Weeks 4 5irfanaNo ratings yet
- Rights As Bribes ResaltadoDocument89 pagesRights As Bribes ResaltadoAndresAmarillaNo ratings yet
- Heirs of Candelaria V RomeroDocument2 pagesHeirs of Candelaria V Romeromoniquehadjirul100% (1)
- Teacher LOA & TermsDocument3 pagesTeacher LOA & TermsMike SchmoronoffNo ratings yet
- Physical Education: Learning Activity SheetDocument13 pagesPhysical Education: Learning Activity SheetRhea Jane B. CatalanNo ratings yet
- The Prodigious MuseDocument466 pagesThe Prodigious Musesleepyninjitsu100% (1)
- Labor Law Review Questions and AnswersDocument151 pagesLabor Law Review Questions and AnswersCarty MarianoNo ratings yet
- Srs For College WebsiteDocument6 pagesSrs For College WebsiteShree Kumar33% (3)
- Revised Market Making Agreement 31.03Document13 pagesRevised Market Making Agreement 31.03Bhavin SagarNo ratings yet
- RBG - CRM BRD - Marketing - v4.1Document68 pagesRBG - CRM BRD - Marketing - v4.1Manvi Pareek100% (2)
- The First Converts in Chin Hills - Ni Kong HongDocument7 pagesThe First Converts in Chin Hills - Ni Kong HongLTTuangNo ratings yet
- The Utopia of The Zero-OptionDocument25 pagesThe Utopia of The Zero-Optiontamarapro50% (2)
- Redemption and The Relief Work RevisedDocument234 pagesRedemption and The Relief Work RevisedYewo Humphrey MhangoNo ratings yet
- Grade 3 MathematicsDocument3 pagesGrade 3 Mathematicsailaine grace alapNo ratings yet
- Chapter 15 NegotiationsDocument16 pagesChapter 15 NegotiationsAdil HayatNo ratings yet
- Average and Instantaneous AccelerationDocument35 pagesAverage and Instantaneous AccelerationaraneyaNo ratings yet
- Cri 192Document5 pagesCri 192Reyn CagmatNo ratings yet
- Business Finance Chapter 4Document15 pagesBusiness Finance Chapter 4chloe frostNo ratings yet
- Dnyanadeep's IAS: UPSC Essay Series - 7Document2 pagesDnyanadeep's IAS: UPSC Essay Series - 7Rahul SinghNo ratings yet
- Midterm Examination: General MathematicsDocument5 pagesMidterm Examination: General MathematicsJenalyn CardanoNo ratings yet
- ShakespeareDocument12 pagesShakespeareapi-510189551No ratings yet
- Project BBADocument77 pagesProject BBAShivamNo ratings yet
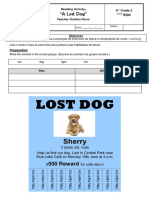
- Reading Activity - A Lost DogDocument3 pagesReading Activity - A Lost DogGigsFloripaNo ratings yet
- WWW Foboko Com Sentence Dictionary English UnderstandDocument12 pagesWWW Foboko Com Sentence Dictionary English UnderstandEnkhee WefweeNo ratings yet
- POWEV2434234Document461 pagesPOWEV2434234John M. HemsworthNo ratings yet
- Advanced Finite Element Model of Tsing Ma Bridge For Structural Health MonitoringDocument32 pagesAdvanced Finite Element Model of Tsing Ma Bridge For Structural Health MonitoringZhang ChaodongNo ratings yet