You might also like
- Pathophysiology ACS AMIDocument8 pagesPathophysiology ACS AMIRichelle Pancho PunayNo ratings yet
- Pathophysiology ACS AMIDocument8 pagesPathophysiology ACS AMIRichelle Pancho PunayNo ratings yet
- Acs 2Document8 pagesAcs 2Richelle Pancho PunayNo ratings yet
- Acs 2Document8 pagesAcs 2Richelle Pancho PunayNo ratings yet
- Acs 2Document8 pagesAcs 2Richelle Pancho PunayNo ratings yet
- Acute Pain Secondary To TiDocument3 pagesAcute Pain Secondary To TiRichelle Pancho PunayNo ratings yet
- Pa ThoDocument1 pagePa ThoRichelle Pancho PunayNo ratings yet
- Acute Pain Secondary To TiDocument3 pagesAcute Pain Secondary To TiRichelle Pancho PunayNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Board Questions in PharmacologyDocument12 pagesBoard Questions in PharmacologyJo Anne100% (6)
- The World Drug Report - Executive Summary Chapter 1: Trends in World Drug Markets EvolutionDocument21 pagesThe World Drug Report - Executive Summary Chapter 1: Trends in World Drug Markets EvolutionlosangelesNo ratings yet
- 1 - Ocular TraumaDocument31 pages1 - Ocular TraumadeoshiNo ratings yet
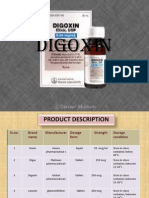
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- Drugs For Circulatory DisordersDocument32 pagesDrugs For Circulatory Disordersnk999999No ratings yet
- Excipient Risk Assessment-Possible Approaches To Assessing The Risk Associated With Excipient FunctionDocument9 pagesExcipient Risk Assessment-Possible Approaches To Assessing The Risk Associated With Excipient FunctionАнна ОрлеоглоNo ratings yet
- Daftar Obat High AlertDocument31 pagesDaftar Obat High Alertmuin ritongaNo ratings yet
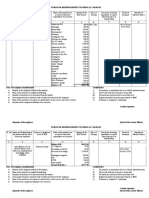
- Medical BillDocument8 pagesMedical Billsarveshfdk48No ratings yet
- Pediatric DentistryDocument15 pagesPediatric DentistryPeyman Dhg100% (2)
- Farmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiDocument19 pagesFarmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiCici MastaNo ratings yet
- ToxicologyDocument2 pagesToxicologyTOD100% (1)
- Case Study - Novartis V UOI PDFDocument15 pagesCase Study - Novartis V UOI PDFRaGa JoThiNo ratings yet
- AU NZ Cortitrol PIPDocument2 pagesAU NZ Cortitrol PIPthanh.tkNo ratings yet
- Case 11 AsthmaDocument131 pagesCase 11 Asthmaspajda69No ratings yet
- Van de Wiele 01 PDFDocument36 pagesVan de Wiele 01 PDFbiraj majumderNo ratings yet
- BrianamedlinotcbirthcontrolDocument5 pagesBrianamedlinotcbirthcontrolapi-251698471No ratings yet
- Patent Overview and Human Rights in The Light of Novartis Case 130628050722 Phpapp02Document19 pagesPatent Overview and Human Rights in The Light of Novartis Case 130628050722 Phpapp02hardika putraNo ratings yet
- Caffeine HistoryDocument9 pagesCaffeine HistoryWynona Genesis G. BasilioNo ratings yet
- CapsulesDocument60 pagesCapsulesprinceamitNo ratings yet
- Alan Anderson Bangun 22010110120053 Bab8ktiDocument18 pagesAlan Anderson Bangun 22010110120053 Bab8ktiErvan PrasetiyoNo ratings yet
- Sample Calculation Problems With AnswerDocument7 pagesSample Calculation Problems With AnswerStephen Gabriel BongolNo ratings yet
- Introduction PharmaceuticsDocument9 pagesIntroduction PharmaceuticsVIJAY KUMAR TIRUKKACHINo ratings yet
- Drug StudyDocument4 pagesDrug StudyHarold Dave IgcalinosNo ratings yet
- Manufacturing of Tablets by Direct Compression Method - Reader ViewDocument1 pageManufacturing of Tablets by Direct Compression Method - Reader ViewMarta HalimNo ratings yet
- 8 Review of Related Literature RRLDocument16 pages8 Review of Related Literature RRLRome Empe BalNo ratings yet
- NCLEX FundamentalsDocument13 pagesNCLEX FundamentalsSara Pirman100% (1)
- Penny Stretcher 04/08/2015Document45 pagesPenny Stretcher 04/08/2015Sherman Publications, Inc.No ratings yet
- Phebra-Sodium Nitrite Inj 3% (Antidote SDocument3 pagesPhebra-Sodium Nitrite Inj 3% (Antidote SmirsupiusmanNo ratings yet
- CinacalcetDocument4 pagesCinacalcetSorina HermanNo ratings yet
- Pharmacology of Opioid AnalgesicsDocument64 pagesPharmacology of Opioid AnalgesicsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)