You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Harvard School of Public Health Health and Society Ph201X Instructors Faculty Lead: Ichiro Kawachi, MD, PHDDocument8 pagesHarvard School of Public Health Health and Society Ph201X Instructors Faculty Lead: Ichiro Kawachi, MD, PHDmarkkkkkkkheeessNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- 1 PDFDocument77 pages1 PDFmarkkkkkkkheeessNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 16 WHO Health Systems Financing WDR 2010Document12 pages16 WHO Health Systems Financing WDR 2010markkkkkkkheeessNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Sample Academic MEMODocument1 pageSample Academic MEMOmarkkkkkkkheeessNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ra 10354 PDFDocument24 pagesRa 10354 PDFmarkkkkkkkheeessNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Abstract Submission Form 2018 PPA ConferenceDocument2 pagesAbstract Submission Form 2018 PPA ConferencemarkkkkkkkheeessNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 05 Yasuhiko Saito Japanese Longitudinal Study of AgingDocument79 pages05 Yasuhiko Saito Japanese Longitudinal Study of AgingmarkkkkkkkheeessNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Introduction and Overview: Data Scientist: The Sexiest Job of The 21st CenturyDocument13 pagesIntroduction and Overview: Data Scientist: The Sexiest Job of The 21st CenturymarkkkkkkkheeessNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
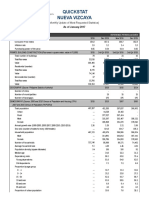
- Quickstat Nueva Vizcaya: (Monthly Update of Most Requested Statistics)Document5 pagesQuickstat Nueva Vizcaya: (Monthly Update of Most Requested Statistics)markkkkkkkheeessNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Lecture16 PDFDocument27 pagesLecture16 PDFmarkkkkkkkheeessNo ratings yet
- 101 Health Research Template Ethical ConsiderationsDocument2 pages101 Health Research Template Ethical ConsiderationsmarkkkkkkkheeessNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Continuous Data MeasuresDocument16 pagesContinuous Data MeasuresmarkkkkkkkheeessNo ratings yet
- Independent Variables Living ArrangementDocument1 pageIndependent Variables Living ArrangementmarkkkkkkkheeessNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Test Bank For Medical Terminology Simplified A Programmed Learning Approach by Body System 5th Edition Barbara A Gylys Regina M Masters IsDocument15 pagesTest Bank For Medical Terminology Simplified A Programmed Learning Approach by Body System 5th Edition Barbara A Gylys Regina M Masters Isuntoldvasculumcj4e5cNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Moodiness in ADHD. A Clinician Guide PDFDocument193 pagesMoodiness in ADHD. A Clinician Guide PDFCristina100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Disease and Disease TransmissionDocument48 pagesDisease and Disease TransmissionAYO NELSONNo ratings yet
- The Radiology Assistant - Bi-RADS For Mammography and Ultrasound 2013Document29 pagesThe Radiology Assistant - Bi-RADS For Mammography and Ultrasound 2013shail0143No ratings yet
- Capstone ProjectDocument11 pagesCapstone ProjectDave Matthew LibiranNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- GTD Case StudyDocument9 pagesGTD Case StudyZnarf Izlah Sadanreb100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- C Reactive ProteinDocument24 pagesC Reactive ProteinMohammed FareedNo ratings yet
- Seminar ImnciDocument15 pagesSeminar Imnciseema devassy100% (1)
- HistologyDocument15 pagesHistologySara ŠvedekNo ratings yet
- Malaria Control ProgramDocument74 pagesMalaria Control ProgramMary Ruth Aujero Sanchez-Benzon100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Psychosis and Memory Loss by Dr. Shivan MahabirDocument41 pagesPsychosis and Memory Loss by Dr. Shivan MahabirShivan A.C.No ratings yet
- PicaDocument10 pagesPicafelinndNo ratings yet
- DRUG - STUDY CeferuximeDocument6 pagesDRUG - STUDY Ceferuximepius troy macapazNo ratings yet
- Telegram@DrbooksDocument493 pagesTelegram@DrbooksDanh Nguyễn100% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Imaging of Solitary and Multiple Pulmonary NodulesDocument75 pagesImaging of Solitary and Multiple Pulmonary NodulesAnshulVarshneyNo ratings yet
- Homeostasis and The Excretory SystemDocument21 pagesHomeostasis and The Excretory Systemmark smithNo ratings yet
- Maternal and Child Health Programmes: MCH ServicesDocument10 pagesMaternal and Child Health Programmes: MCH ServicesRosebel LaguraNo ratings yet
- HydrotherapyDocument40 pagesHydrotherapyThopu UmamaheswariNo ratings yet
- Mandibular Nerve Block (Other Techniques)Document24 pagesMandibular Nerve Block (Other Techniques)daw022100% (2)
- Relapsing Polychondritis Case Presentaion Feb 2009 DR - BugnahDocument21 pagesRelapsing Polychondritis Case Presentaion Feb 2009 DR - BugnahDr.Sherif Bugnah100% (4)
- SBAR Communication Form: and Progress NoteDocument3 pagesSBAR Communication Form: and Progress NoteTisa Meriel100% (1)
- Humoral ImmunityDocument86 pagesHumoral ImmunitySinthiya KanesaratnamNo ratings yet
- Janet RowleyDocument1 pageJanet RowleyANA GABRIELA PEREZ VIDALNo ratings yet
- Fetal Distress Day 1Document16 pagesFetal Distress Day 1day dayu100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- M.O.S DismantlingDocument18 pagesM.O.S DismantlingAhmed Khaled100% (1)
- Tutorial Klinik: Widyarto Nugroho Pembimbing: Dr. M. Agung Pramudjito, SP - PDDocument73 pagesTutorial Klinik: Widyarto Nugroho Pembimbing: Dr. M. Agung Pramudjito, SP - PDPutri PermataNo ratings yet
- The Role of Acute Phase Proteins in Diagnosis and ManagementDocument6 pagesThe Role of Acute Phase Proteins in Diagnosis and ManagementCabinet VeterinarNo ratings yet
- Abatacept Hervey2006Document9 pagesAbatacept Hervey2006Calvin Tanuwijaya Stick BolaNo ratings yet
- Argumentative Essay: Why The COVID-19 Vaccine Should Be MandatedDocument10 pagesArgumentative Essay: Why The COVID-19 Vaccine Should Be MandatedJulia Brok100% (1)
- Presentation 1Document36 pagesPresentation 1madhurima kunduNo ratings yet