You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
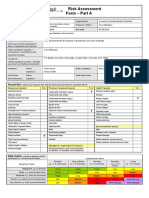
- Risk AssessmentDocument2 pagesRisk AssessmentFaraiMbudaya0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Polymer CharacterizationDocument29 pagesPolymer CharacterizationCarlos Miguel Dacaimat0% (1)
- Experiment 2 - Study of Packed Column DistillationDocument7 pagesExperiment 2 - Study of Packed Column DistillationAdawiyah Az-zahra100% (1)
- ReportDocument20 pagesReportAidaFarzanaNanaNo ratings yet
- A Sustainable Bioplastic Obtained From Rice StrawDocument12 pagesA Sustainable Bioplastic Obtained From Rice StrawNovrynda Eko SatriawanNo ratings yet
- Calcium and Magnesium Determinations by EDTA Titrations1 (Soil Science Society of America Journal, Vol. 25, Issue 1) (1961)Document3 pagesCalcium and Magnesium Determinations by EDTA Titrations1 (Soil Science Society of America Journal, Vol. 25, Issue 1) (1961)Heba TahaNo ratings yet
- Sampling Procedure For Impact Testing of Structural SteelDocument5 pagesSampling Procedure For Impact Testing of Structural Steelrodrigo nuñezNo ratings yet
- Final Exam in PhysicsDocument5 pagesFinal Exam in Physicsmvmbapple0% (1)
- Carbohydrate Qualitative AnalysisDocument9 pagesCarbohydrate Qualitative AnalysisRamesh KandagatlaNo ratings yet
- Gases AnswersDocument8 pagesGases AnswersSayNo ratings yet
- The Strange Case of Mole Airlines Flight 1023: Preib/Ap Chemistry - Unit 5 Chemical QuantitiesDocument7 pagesThe Strange Case of Mole Airlines Flight 1023: Preib/Ap Chemistry - Unit 5 Chemical QuantitiesGiordi Emmanuel SalinasNo ratings yet
- Ch. 15 Review AnswersDocument2 pagesCh. 15 Review AnswersJose PopoffNo ratings yet
- LTC Curvas en OriginDocument15 pagesLTC Curvas en OriginDiego CorreaNo ratings yet
- Elvis 4Document9 pagesElvis 4Azhar Ali Zafar0% (1)
- 9701 w05 QP 4Document12 pages9701 w05 QP 4Hubbak KhanNo ratings yet
- Centrifugal PumpsDocument26 pagesCentrifugal PumpsromwamaNo ratings yet
- ACCDocument18 pagesACCSanchit AgarwalNo ratings yet
- Density of KOH SolutionsDocument1 pageDensity of KOH SolutionsjohnihaasNo ratings yet
- Laboratory ManualDocument13 pagesLaboratory ManualPaul UyNo ratings yet
- Shear Wall Modelling Techniques: A ReviewDocument9 pagesShear Wall Modelling Techniques: A ReviewAmanulla MullaNo ratings yet
- Inform Energy Sanicube InformationDocument11 pagesInform Energy Sanicube Informationh2odavidNo ratings yet
- The Tin-God's DrumsDocument4 pagesThe Tin-God's DrumsDonald Robinson100% (1)
- Astm C 171-07Document2 pagesAstm C 171-07jun floresNo ratings yet
- Análisis de Textura en Frutas CongeladasDocument9 pagesAnálisis de Textura en Frutas CongeladasJORGENo ratings yet
- Refrigerator Test R1Document9 pagesRefrigerator Test R1GHyukendo Shaddiq AkhbarNo ratings yet
- Mrex - Brochure 0810 PDFDocument12 pagesMrex - Brochure 0810 PDFGyörgy BernáthNo ratings yet
- 10 - Chapter 2 PDFDocument72 pages10 - Chapter 2 PDFAwais SargodianNo ratings yet
- Herb-Modle Peptide in Anaerobic Titration and Reduce-05032013Document4 pagesHerb-Modle Peptide in Anaerobic Titration and Reduce-05032013陳育孝No ratings yet
- Ls Series Washer Extractors: Designed To LastDocument4 pagesLs Series Washer Extractors: Designed To LastTom DavidcsNo ratings yet
- Assignment For Iupac Nomenclature: CH - CH-CH - CHDocument5 pagesAssignment For Iupac Nomenclature: CH - CH-CH - CHapi-233404189No ratings yet