You might also like
- Antidepressant DrugsDocument21 pagesAntidepressant DrugsKashis SharmaNo ratings yet
- AntidepressantsDocument5 pagesAntidepressantsUm HamoOd100% (2)
- Antidepressants MaterialDocument5 pagesAntidepressants MaterialxyzNo ratings yet
- Anti Depressants FinalDocument61 pagesAnti Depressants FinalAuthor Nauman Shad100% (1)
- Psychopharmacology 2 AntidepressantsDocument7 pagesPsychopharmacology 2 AntidepressantsBea Samonte100% (2)
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- Preferentially Block Uptake of 5-HT Preferentially Block Uptake of NADocument3 pagesPreferentially Block Uptake of 5-HT Preferentially Block Uptake of NAThư Phạm100% (1)
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Revellionz'19 - Second Year Question BankDocument114 pagesRevellionz'19 - Second Year Question BankRamNo ratings yet
- PA 644 - M2 LecturesDocument412 pagesPA 644 - M2 LectureskatNo ratings yet
- Antidepressants and AntipsychoticsDocument50 pagesAntidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Overview of Psychotropic DrugsDocument7 pagesOverview of Psychotropic Drugsnad101No ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- Psychopharmacology 1Document7 pagesPsychopharmacology 1RajP01No ratings yet
- Neuroleptics & AnxiolyticsDocument65 pagesNeuroleptics & AnxiolyticsAntonPurpurovNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- AntidepressantsDocument59 pagesAntidepressantsanon_189054600100% (2)
- Medication Fact Book for Psychiatric Practice, Fifth EditionFrom EverandMedication Fact Book for Psychiatric Practice, Fifth EditionNo ratings yet
- The Wiley-Blackwell Handbook of Addiction PsychopharmacologyFrom EverandThe Wiley-Blackwell Handbook of Addiction PsychopharmacologyNo ratings yet
- The Maudsley Prescribing Guidelines in PsychiatryFrom EverandThe Maudsley Prescribing Guidelines in PsychiatryRating: 4 out of 5 stars4/5 (1)
- AntipsychoticsDocument10 pagesAntipsychoticswawing16No ratings yet
- Psychopharmacology in PsychiatryDocument94 pagesPsychopharmacology in PsychiatryOslo SaputraNo ratings yet
- (OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Document16 pages(OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Yavuz DanisNo ratings yet
- Adrenergic AgentsDocument57 pagesAdrenergic AgentsAn Lo100% (1)
- DOPAMINE SYN, TRAN, DEGR and ReceptorsDocument15 pagesDOPAMINE SYN, TRAN, DEGR and ReceptorsRaghuram MiryalaNo ratings yet
- Substance Use DisordersDocument28 pagesSubstance Use DisordersAbdul NazarNo ratings yet
- Pharmacotherapy in PschiatryDocument8 pagesPharmacotherapy in PschiatryygfhdgNo ratings yet
- AntiemeticsDocument25 pagesAntiemeticsPridho GaziansyahNo ratings yet
- AnxietyDocument5 pagesAnxietyJohn HolmesNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Psychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthDocument72 pagesPsychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthMichael Urrutia100% (2)
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 pagesCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNo ratings yet
- Mental Health and Psychiatric Nursing: Vernalin B. Terrado, RNDocument35 pagesMental Health and Psychiatric Nursing: Vernalin B. Terrado, RNverna100% (1)
- INTRODUCTION TO NEUROPHARMACOLOGYyyDocument27 pagesINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviNo ratings yet
- Biological Aspects of OCD SeminarDocument60 pagesBiological Aspects of OCD Seminarneha mattikoppaNo ratings yet
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- Antidepressant Side Effects 2006Document9 pagesAntidepressant Side Effects 2006Renny AnggrainiNo ratings yet
- Drugs For NeurolepticsDocument1 pageDrugs For Neurolepticssyamil_daudNo ratings yet
- Pharmacology Medical Suffixes Cheat SheetDocument1 pagePharmacology Medical Suffixes Cheat SheetPattyNo ratings yet
- Module 3 - D - Antipsychotics For Bipolar DisorderDocument19 pagesModule 3 - D - Antipsychotics For Bipolar Disorderpsychopharmacology100% (2)
- Sedative HypnoticsDocument41 pagesSedative HypnoticsPatrick Juacalla100% (2)
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonNo ratings yet
- Drug List Psych Optho NeuroDocument22 pagesDrug List Psych Optho NeuroAshley BarrileNo ratings yet
- Enzyme Inducers & InhibitorsDocument1 pageEnzyme Inducers & InhibitorsM. JoyceNo ratings yet
- Adrenergic AntagonistsDocument6 pagesAdrenergic Antagonistsfiena92100% (2)
- 4.2 Psychotropic Drugs Used in PsychiatryDocument32 pages4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliNo ratings yet
- Antipsychotics: Corina Freitas MS, MD, MBA, DABFMDocument48 pagesAntipsychotics: Corina Freitas MS, MD, MBA, DABFMCorina FreitasNo ratings yet
- Biological Bases Study GuideDocument13 pagesBiological Bases Study Guideapi-421695293No ratings yet
- Psychopharma 1Document7 pagesPsychopharma 1Mitchee Zialcita100% (1)
- Table 1: Substrates of Cytochrome P450 (CYP) EnzymesDocument6 pagesTable 1: Substrates of Cytochrome P450 (CYP) EnzymesNurul Kamilah SadliNo ratings yet
- Sedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeDocument347 pagesSedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeEsha pantNo ratings yet
- Daftar Obat Praktik DokterDocument5 pagesDaftar Obat Praktik DokterRandy WinataNo ratings yet
- Rincian Pembelian 2020Document55 pagesRincian Pembelian 2020irwan es ye teNo ratings yet
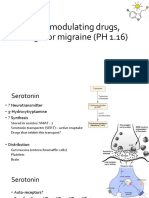
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Document13 pages5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNo ratings yet
- Tapering BenzodiazepinesDocument3 pagesTapering BenzodiazepineslgiuzfgukuzfglufzNo ratings yet
- List of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)Document7 pagesList of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)mcamilaarredondovelezNo ratings yet
- Crocin Syrup - Google SearchDocument1 pageCrocin Syrup - Google Searchbhagwati bombNo ratings yet
- Daftar Obat Dokter AnakDocument2 pagesDaftar Obat Dokter AnakAnonymous gec5CIKoNo ratings yet
- Opoid AnalgesicsDocument48 pagesOpoid AnalgesicsPratik KhanalNo ratings yet
- UPDATED Handout - PHARMA - DR. GRAGEDADocument238 pagesUPDATED Handout - PHARMA - DR. GRAGEDApasabay270No ratings yet
- Xtampza Vs Oxycontin - Main Differences and SimilaritiesDocument4 pagesXtampza Vs Oxycontin - Main Differences and SimilaritiesNicholas FeatherstonNo ratings yet
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDocument10 pagesRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFAnonymous idPPyERfBnNo ratings yet
- NCLEX PsychiatryDocument55 pagesNCLEX PsychiatryYaoling WenNo ratings yet
- Sedatives & HypnoticsDocument25 pagesSedatives & HypnoticsBharat MakwanaNo ratings yet
- MDTH: Mood Disorders Treatment History FormDocument3 pagesMDTH: Mood Disorders Treatment History FormLaura ParkaNo ratings yet
- Daftar Harga Generik Galaxy 3 PT. Hexpharm Jaya Divisi OGB Per 25 Maret 2019 Kode Baru & Perubahan HNA+DiscDocument1 pageDaftar Harga Generik Galaxy 3 PT. Hexpharm Jaya Divisi OGB Per 25 Maret 2019 Kode Baru & Perubahan HNA+DiscnadarNo ratings yet
- Module 10-NSTP 1 - Drug Abuse and PreventionDocument24 pagesModule 10-NSTP 1 - Drug Abuse and PreventionLalaine Alon100% (1)
- RDL Alpha List PDFDocument127 pagesRDL Alpha List PDFmdaihNo ratings yet
- Drug-Induced Serotonin Syndrome - A ReviewDocument10 pagesDrug-Induced Serotonin Syndrome - A ReviewAshrafNo ratings yet
- Drug Abuse PreventionDocument1 pageDrug Abuse PreventionAllain ChristopherNo ratings yet
- Daftar Obat Narkotika: NO Nama SatuanDocument5 pagesDaftar Obat Narkotika: NO Nama Satuanhernandi denkgNo ratings yet
- Levomepromazine Drug StudyDocument2 pagesLevomepromazine Drug Studykint manlangitNo ratings yet
- PREGABALINDocument5 pagesPREGABALINJojenelle R. TepaitNo ratings yet
- H01043 Hoá Dư C 2 Lecture 8 Antipsychotic DrugsDocument24 pagesH01043 Hoá Dư C 2 Lecture 8 Antipsychotic DrugsKTrọng NghĩaNo ratings yet
- Psychiatry Divine InterventionDocument44 pagesPsychiatry Divine InterventionDEEJKNo ratings yet
- by DEA Drug Code Number - : Controlled SubstancesDocument16 pagesby DEA Drug Code Number - : Controlled Substanceslumik1234No ratings yet
- PrescriptionDocument2 pagesPrescriptionSaif AliNo ratings yet
- Metoclopramide (Reglan)Document1 pageMetoclopramide (Reglan)ENo ratings yet
- Patient Retrospective FormDocument1 pagePatient Retrospective FormLuis Juárez GtzNo ratings yet
- Type Drug ChartDocument3 pagesType Drug ChartKarina Rodriguez100% (3)