You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GCAF Online Inspector Practice ExamDocument5 pagesGCAF Online Inspector Practice Examcamwills2100% (1)
- Watson Studio - IBM CloudDocument2 pagesWatson Studio - IBM CloudPurvaNo ratings yet
- Ye Zindagi Aur Mujhe Fanaa KardeDocument9 pagesYe Zindagi Aur Mujhe Fanaa Kardeankur9359saxenaNo ratings yet
- Ball Bearings 1Document17 pagesBall Bearings 1ManicharanNo ratings yet
- EM24DINDSDocument14 pagesEM24DINDSJavaprima Dinamika AbadiNo ratings yet
- 2021.01 - Key-Findings - Green Bond Premium - ENDocument6 pages2021.01 - Key-Findings - Green Bond Premium - ENlypozNo ratings yet
- Family Nursing Care PlanDocument2 pagesFamily Nursing Care PlanSophia Ella OnanNo ratings yet
- Ratio, Proportion, and Percent: Presented By: John Darryl M. Genio Bocobo #3Document18 pagesRatio, Proportion, and Percent: Presented By: John Darryl M. Genio Bocobo #3John Darryl GenioNo ratings yet
- 7-Seater MPV: Kia SingaporeDocument16 pages7-Seater MPV: Kia SingaporeadiNo ratings yet
- VPN Risk Report Cybersecurity InsidersDocument20 pagesVPN Risk Report Cybersecurity InsidersMaria PerezNo ratings yet
- Hevc StandardDocument11 pagesHevc Standardganesh gangatharanNo ratings yet
- Chapter 2 (Teacher)Document19 pagesChapter 2 (Teacher)ajakazNo ratings yet
- Regenerative Braking System: An Efficient Way to Conserve EnergyDocument31 pagesRegenerative Braking System: An Efficient Way to Conserve EnergyPRAVIN KUMAR NNo ratings yet
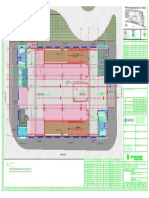
- Key plan and area statement comparison for multi-level car park (MLCPDocument1 pageKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYANo ratings yet
- 28 GHZ Millimeter Wave Cellular Communication Measurements For Reflection and Penetration Loss in and Around Buildings in New York CityDocument5 pages28 GHZ Millimeter Wave Cellular Communication Measurements For Reflection and Penetration Loss in and Around Buildings in New York CityJunyi LiNo ratings yet
- Sales TAX FORMATDocument6 pagesSales TAX FORMATMuhammad HamzaNo ratings yet
- English Assignment AnswersDocument4 pagesEnglish Assignment AnswersAfidaNo ratings yet
- A 231 - A 231M - 15 PDFDocument4 pagesA 231 - A 231M - 15 PDFأسامة وحيد الدين رمضانNo ratings yet
- GI Tags Complete ListDocument17 pagesGI Tags Complete Listrameshb87No ratings yet
- Organic FertilizerDocument2 pagesOrganic FertilizerBien Morfe67% (3)
- Ashok LeylandDocument4 pagesAshok Leylandsodhiseema100% (1)
- Martek Navgard BnwasDocument4 pagesMartek Navgard BnwasСергей БородинNo ratings yet
- Examen 03 Aula - F PostgradoDocument5 pagesExamen 03 Aula - F PostgradodiegoNo ratings yet
- Geography Lesson PlanDocument4 pagesGeography Lesson Planapi-204977805100% (3)
- Grade 5 PPT English Q4 W3 Day 2Document17 pagesGrade 5 PPT English Q4 W3 Day 2Rommel MarianoNo ratings yet
- Cylinder Liner W32Document1 pageCylinder Liner W32Poma100% (1)
- Hocketts Features of Human Language Zed and JasDocument41 pagesHocketts Features of Human Language Zed and JasRechelle Marmol100% (1)
- R-101 and D-101 energy balancesDocument4 pagesR-101 and D-101 energy balancesPuteri MimieNo ratings yet
- The Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Document31 pagesThe Muscle and Strength Training Pyramid v2.0 Training by Eric Helms-9Hamada MansourNo ratings yet
- Tutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesDocument39 pagesTutorial Letter 101/3/2018: Internal Auditing: Theory & PrinciplesSAMANTHANo ratings yet