You might also like
- CURRICULUM VITAE Kham Khan Suan Hausing, PHDDocument8 pagesCURRICULUM VITAE Kham Khan Suan Hausing, PHDCinpu ZomiNo ratings yet
- Moon and SaturnDocument4 pagesMoon and SaturnRamanasarmaNo ratings yet
- WWW - Ib.academy: Study GuideDocument122 pagesWWW - Ib.academy: Study GuideHendrikEspinozaLoyola100% (2)
- Appellees Brief CIVILDocument7 pagesAppellees Brief CIVILBenBulacNo ratings yet
- Dr. Adeel Ahmed Waheed: House Officer M-4Document84 pagesDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNo ratings yet
- Osteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of ChittagongDocument30 pagesOsteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of Chittagongsamiul bashirNo ratings yet
- Quarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The PhilippinesDocument21 pagesQuarter 2-Module 7 Social and Political Stratification: Department of Education Republic of The Philippinestricia100% (5)
- Epic Story of IbalonDocument30 pagesEpic Story of IbalonKi Ko100% (3)
- Who, Summary NotesDocument12 pagesWho, Summary NotesIvan Lohr100% (2)
- Parkinson DiseaseDocument49 pagesParkinson Diseaseiqra100% (1)
- Introduction To E-Business SystemsDocument19 pagesIntroduction To E-Business SystemsArtur97% (79)
- Approach To Unconsious PTDocument62 pagesApproach To Unconsious PTHussain AzharNo ratings yet
- Case Presentation ParaplegiaDocument51 pagesCase Presentation ParaplegiaHussain Azhar100% (2)
- Assignment Submission Form: Pgid Name of The MemberDocument9 pagesAssignment Submission Form: Pgid Name of The MemberNamit GaurNo ratings yet
- Emergency Room Drug ListDocument28 pagesEmergency Room Drug Listiscariot02No ratings yet
- Analysing Worship in The Pentateuch and Its ApplicationDocument12 pagesAnalysing Worship in The Pentateuch and Its ApplicationDaniel Solomon100% (1)
- Drug Study-Sodium BicarbonateDocument7 pagesDrug Study-Sodium BicarbonateTrisha Faye OrtegaNo ratings yet
- Uterine Myoma Case Study Group A FinalDocument88 pagesUterine Myoma Case Study Group A Finallowell cerezoNo ratings yet
- NCP DM and HCVDDocument3 pagesNCP DM and HCVDMAYBELINE OBAOB100% (1)
- Case Study Final PortraitDocument11 pagesCase Study Final PortraitZhy CaluzaNo ratings yet
- PantoprazoleDocument1 pagePantoprazolehahahahaaaaaaaNo ratings yet
- Drug StudyDocument13 pagesDrug StudyAldrin Ian Oraza AlpeNo ratings yet
- Drug Study FinalDocument6 pagesDrug Study FinalJade HemmingsNo ratings yet
- BaclofenDocument2 pagesBaclofenamiraNo ratings yet
- NCP Episiotomy WoundDocument3 pagesNCP Episiotomy WoundJP2001No ratings yet
- Drug LovenoxDocument2 pagesDrug LovenoxSrkocherNo ratings yet
- Peros: General AssessmentDocument4 pagesPeros: General AssessmentKaycee TolingNo ratings yet
- Chart View Admission Lab WorkDocument4 pagesChart View Admission Lab Workania ojedaNo ratings yet
- A Client With Cushing's Syndrome: Nursing Care PlanDocument1 pageA Client With Cushing's Syndrome: Nursing Care PlanJulius Caesar ColladoNo ratings yet
- Cellulitis Discharge PlanDocument1 pageCellulitis Discharge PlanJuvy Rose Tinga YeeNo ratings yet
- Drug Study ColestipolDocument3 pagesDrug Study ColestipolAbby AngNo ratings yet
- Cefixime: Suprax Class and CategoryDocument3 pagesCefixime: Suprax Class and CategoryArianne Joy SalvadorNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddleNo ratings yet
- Altretamine: Drug DosageDocument16 pagesAltretamine: Drug DosagePrincess CruzNo ratings yet
- Case 1Document9 pagesCase 1Joselyn M. LachicaNo ratings yet
- Dolan Drug StudyDocument3 pagesDolan Drug StudyLian Robbie BautistaNo ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDocument4 pagesTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNo ratings yet
- Example of Drug StudyDocument2 pagesExample of Drug Studydonna mae junioNo ratings yet
- Vitamin KDocument2 pagesVitamin KMuvs RazonNo ratings yet
- MannitolDocument3 pagesMannitolAlexandra AntondyNo ratings yet
- HEMARATE FA Hemarate FA Consists of Folic AcidDocument2 pagesHEMARATE FA Hemarate FA Consists of Folic AcidMarhina Asarabi MukimNo ratings yet
- KaliumDocument2 pagesKaliumJustine Kaye Iballa HarligaNo ratings yet
- Drug StudyDocument9 pagesDrug StudyShane Arroyo100% (1)
- Discharge PlanDocument1 pageDischarge PlanBernalene SyNo ratings yet
- Co DiovanDocument2 pagesCo DiovanianecunarNo ratings yet
- Week 3. COURSE TASK - Acute PancreatitisDocument3 pagesWeek 3. COURSE TASK - Acute PancreatitisqwertNo ratings yet
- Miglitol (Glyset)Document1 pageMiglitol (Glyset)ENo ratings yet
- RevisionDocument17 pagesRevisionMatt RenaudNo ratings yet
- LOVASTATINDocument2 pagesLOVASTATINAngel CatalanNo ratings yet
- Obat ObgynDocument8 pagesObat ObgynMuhammad Naqiuddin JalaluddinNo ratings yet
- Vit B1 ReportDocument19 pagesVit B1 ReportNatasha Faye UntalanNo ratings yet
- CetirizineDocument2 pagesCetirizinelintangNo ratings yet
- ICS Pedia WardDocument8 pagesICS Pedia Wardsweet061991No ratings yet
- IFOSFAMIDEDocument4 pagesIFOSFAMIDEErza GenatrikaNo ratings yet
- From Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsDocument2 pagesFrom Chronic To Critical: A Latino Family Confronts End-of-Life DecisionsRoyKimNo ratings yet
- Alendronic AcidDocument1 pageAlendronic AcidRPh Krishna Chandra JagritNo ratings yet
- Betahistine Drug InfoDocument3 pagesBetahistine Drug InfoAshish KarnNo ratings yet
- 9 Ketamine Drug StudyDocument7 pages9 Ketamine Drug Studyshadow gonzalezNo ratings yet
- Drug AnalysisDocument3 pagesDrug AnalysisAnn Aquino100% (1)
- Drug StudyDocument5 pagesDrug StudyBridgette ArañesNo ratings yet
- DS (Calcium + Vit. D)Document6 pagesDS (Calcium + Vit. D)Mary April MendezNo ratings yet
- Methyldopa, Losartan K, Ascorbic AcidDocument4 pagesMethyldopa, Losartan K, Ascorbic AcidRico Mae ValenciaNo ratings yet
- Nursing Care Plan On HypertensionDocument5 pagesNursing Care Plan On Hypertensionbhavana100% (1)
- NCP Sa Sinus Tachycardia FinalDocument13 pagesNCP Sa Sinus Tachycardia FinalMYKRISTIE JHO MENDEZNo ratings yet
- Munder Aljanna Marie Nursing Assessment II Part 2 CPDocument3 pagesMunder Aljanna Marie Nursing Assessment II Part 2 CPMohamadhizam M. PangcatanNo ratings yet
- Drug Study Generic Name (Brand Name) Indication Dosage, Route, Frequency Mechanism of Action Adverse Reaction Contraindication Nursing ResponsibilityDocument3 pagesDrug Study Generic Name (Brand Name) Indication Dosage, Route, Frequency Mechanism of Action Adverse Reaction Contraindication Nursing ResponsibilityKimm Charmaine RodriguezNo ratings yet
- ASSESSMENTDocument2 pagesASSESSMENTColeen PequitNo ratings yet
- Darbepoetin AlfaDocument3 pagesDarbepoetin Alfaapi-3797941No ratings yet
- Ferrous SulfateDocument2 pagesFerrous SulfateMiEr Cañas AzenicNo ratings yet
- Drug Study - FurosemideDocument2 pagesDrug Study - FurosemideryanNo ratings yet
- A Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pseudohypoparathyroidism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- Group 2: Magallon, Buenaventura Sallaberger, Jayrahnicole Agliam, Jessica May Diño, FortunatoDocument12 pagesGroup 2: Magallon, Buenaventura Sallaberger, Jayrahnicole Agliam, Jessica May Diño, FortunatoMarinela ManaloNo ratings yet
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
- Anam FinalDocument82 pagesAnam FinalHussain AzharNo ratings yet
- Ion SyndromeDocument67 pagesIon SyndromeHussain AzharNo ratings yet
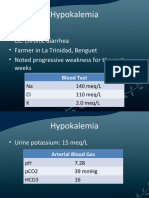
- HypokalemiaDocument12 pagesHypokalemiaMohammad AliNo ratings yet
- Enteric FeverDocument63 pagesEnteric FeverHussain AzharNo ratings yet
- K HomeosDocument47 pagesK HomeosHussain AzharNo ratings yet
- Electrolyte Disturbaces - Hyponatremia and HypernatremiaDocument41 pagesElectrolyte Disturbaces - Hyponatremia and HypernatremiaMohammad AliNo ratings yet
- Dengue 2009Document53 pagesDengue 2009Hussain AzharNo ratings yet
- AntibioticsDocument49 pagesAntibioticsHussain AzharNo ratings yet
- EFFA PRESENTATNhepatic EncephalopathyDocument50 pagesEFFA PRESENTATNhepatic EncephalopathyHussain AzharNo ratings yet
- DVT&PE Final 1Document59 pagesDVT&PE Final 1Hussain AzharNo ratings yet
- DKA Concepts and ManagementDocument22 pagesDKA Concepts and ManagementMohammad AliNo ratings yet
- DVTDocument32 pagesDVTHussain AzharNo ratings yet
- DVT - 2 FaizaDocument65 pagesDVT - 2 FaizaHussain AzharNo ratings yet
- Dka 31-05-11Document52 pagesDka 31-05-11Hussain AzharNo ratings yet
- Copd Final 97-2003hiraaDocument41 pagesCopd Final 97-2003hiraaHussain AzharNo ratings yet
- CP Najma 97Document75 pagesCP Najma 97Hussain AzharNo ratings yet
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocument47 pagesAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNo ratings yet
- Case Presentation 2Document53 pagesCase Presentation 2Hussain AzharNo ratings yet
- An Approach To Anemic PatientDocument79 pagesAn Approach To Anemic PatientHussain AzharNo ratings yet
- AnemiaDocument37 pagesAnemiaHussain AzharNo ratings yet
- Acute Exacerbation of COPDDocument14 pagesAcute Exacerbation of COPDMohammad AliNo ratings yet
- ABG S Final and Last TouchDocument88 pagesABG S Final and Last TouchHussain AzharNo ratings yet
- AKIDocument83 pagesAKIHussain AzharNo ratings yet
- Acute Renal FailureDocument120 pagesAcute Renal FailureHussain AzharNo ratings yet
- Acrf CDocument70 pagesAcrf CHussain AzharNo ratings yet
- DUN Bukit Lanjan CNY Sponsorship Form2Document1 pageDUN Bukit Lanjan CNY Sponsorship Form2alamsekitarselangorNo ratings yet
- 115 FinargDocument294 pages115 FinargMelvin GrijalbaNo ratings yet
- OrthoDocument22 pagesOrthosivaleela gNo ratings yet
- The Machine StopsDocument14 pagesThe Machine StopsMICHAEL HARRIS USITANo ratings yet
- E 18 - 02 - Rte4ltay PDFDocument16 pagesE 18 - 02 - Rte4ltay PDFvinoth kumar SanthanamNo ratings yet
- Match The Animal With Its NameDocument4 pagesMatch The Animal With Its Namekawa kawka kawuniaNo ratings yet
- Southeast Asian Fabrics and AttireDocument5 pagesSoutheast Asian Fabrics and AttireShmaira Ghulam RejanoNo ratings yet
- 15 Melodic Uses of Non-Chord TonesDocument3 pages15 Melodic Uses of Non-Chord TonesonlymusicaNo ratings yet
- Internship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Document57 pagesInternship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Tareq Alam100% (1)
- Man Is Made by His BeliefDocument2 pagesMan Is Made by His BeliefLisa KireechevaNo ratings yet
- A100K10873 VSP-12-Way Technical ManualDocument20 pagesA100K10873 VSP-12-Way Technical Manualchufta50% (2)
- Character Sketch of Elizabeth BennetDocument2 pagesCharacter Sketch of Elizabeth BennetAiman AbdullahNo ratings yet
- Week9 Phylum NemathelminthesDocument26 pagesWeek9 Phylum NemathelminthesCzerinne Angela Justinne AlarillaNo ratings yet
- Tool Stack Template 2013Document15 pagesTool Stack Template 2013strganeshkumarNo ratings yet
- Ang Tibay Vs CADocument2 pagesAng Tibay Vs CAEarl LarroderNo ratings yet
- 3er Grado - DMPA 05 - ACTIVIDAD DE COMPRENSION LECTORA - UNIT 2 - CORRECCIONDocument11 pages3er Grado - DMPA 05 - ACTIVIDAD DE COMPRENSION LECTORA - UNIT 2 - CORRECCIONANDERSON BRUCE MATIAS DE LA SOTANo ratings yet
- Activity Chapter1 ManagementDocument7 pagesActivity Chapter1 ManagementTricia Amigo SacareNo ratings yet
- Behaviour of Investors in Indian Equity Markets: Submitted byDocument26 pagesBehaviour of Investors in Indian Equity Markets: Submitted byDibyanshu AmanNo ratings yet