You might also like
- A Practical Guide To The Management of Impacted Teeth PDFDocument263 pagesA Practical Guide To The Management of Impacted Teeth PDFJaneth García Chávez50% (2)
- A Comparison of Root Resorption Between Invisalign Treatment and Contemporary Orthodontic TreatmentDocument101 pagesA Comparison of Root Resorption Between Invisalign Treatment and Contemporary Orthodontic Treatmentplayer osamaNo ratings yet
- 300 Dental Anatomy Facts VEREY IMPORTNTDocument19 pages300 Dental Anatomy Facts VEREY IMPORTNTOsman SoormaNo ratings yet
- Orthodontic and Non - Orthodontic Root ResorptionDocument8 pagesOrthodontic and Non - Orthodontic Root ResorptionGaurav PoplaiNo ratings yet
- Iatrogenic Effects of Orthodontic TreatmentDocument29 pagesIatrogenic Effects of Orthodontic TreatmentKomal AsifNo ratings yet
- NATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideFrom EverandNATIONAL DENTAL BOARDS (NDB) / PART I: Passbooks Study GuideRating: 1 out of 5 stars1/5 (1)
- Clinical Practice Guidelines - 2017Document54 pagesClinical Practice Guidelines - 2017Cem ÜnsalNo ratings yet
- Reference Range Values For Pediatric Care - Soghier, Lamia M., Pham, Katherine, Rooney, Sara ( (AAP 2014) )Document177 pagesReference Range Values For Pediatric Care - Soghier, Lamia M., Pham, Katherine, Rooney, Sara ( (AAP 2014) )Tan Man100% (4)
- CARIOLOGYDocument77 pagesCARIOLOGYteklay100% (3)
- L G 0014511967 0046781894Document26 pagesL G 0014511967 0046781894anggiNo ratings yet
- MCQ S in Dental MaterialsDocument4 pagesMCQ S in Dental MaterialsSatya AsatyaNo ratings yet
- Tooth Carving Exercise As A Foundation For Future Dental Career - A ReviewDocument3 pagesTooth Carving Exercise As A Foundation For Future Dental Career - A ReviewRik ChatterjeeNo ratings yet
- MCQ in ProsthodonticsDocument5 pagesMCQ in ProsthodonticsMohammed NabeelNo ratings yet
- 09 Dental TechnologyDocument119 pages09 Dental TechnologyVarshapvNo ratings yet
- PMDC UHS 2010 Exam FormatDocument10 pagesPMDC UHS 2010 Exam Formata_friend_in_neeedNo ratings yet
- Teeth Selection For Edentulous CaseDocument29 pagesTeeth Selection For Edentulous CaseFarheen FatimaNo ratings yet
- Topics in Dental BiochemistryDocument322 pagesTopics in Dental BiochemistryjokedulguunNo ratings yet
- Atlas of Oral Histology 2nbsped 9788131254844 8131254844Document143 pagesAtlas of Oral Histology 2nbsped 9788131254844 8131254844Dhikra PikaNo ratings yet
- Comb SyndromeDocument6 pagesComb SyndromemusaabsiddiquiNo ratings yet
- Laboratory Technology Mcq5Document16 pagesLaboratory Technology Mcq5وا إسلاماهNo ratings yet
- Classification of Removable Partial DentureDocument17 pagesClassification of Removable Partial DentureShoaib RaziNo ratings yet
- Basics in Pharmacology For Dental Students - Jaypee Brothers Medical Pub 1 Edition (June 30, 2010)Document524 pagesBasics in Pharmacology For Dental Students - Jaypee Brothers Medical Pub 1 Edition (June 30, 2010)DrleoNo ratings yet
- Lec 5 P 4Document5 pagesLec 5 P 4brshlwnytwaftkhr956No ratings yet
- Anatomy of The Larynx: General DescriptionDocument38 pagesAnatomy of The Larynx: General DescriptionDr-Firas Nayf Al-ThawabiaNo ratings yet
- Dental Anatomy FactsDocument10 pagesDental Anatomy FactsGhee MoralesNo ratings yet
- Development of Dentition & OcclusionDocument109 pagesDevelopment of Dentition & OcclusionSyed Mohammad Osama Ahsan100% (1)
- QRS Jyotsna Rao ProsthoDocument366 pagesQRS Jyotsna Rao Prosthoaditi jhaveriNo ratings yet
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Document27 pagesPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. ZoghborNo ratings yet
- Textbook of Public Health Dentistry 3nbsped 8131246639 9788131246634 CompressDocument522 pagesTextbook of Public Health Dentistry 3nbsped 8131246639 9788131246634 CompressGauri AtwalNo ratings yet
- Success& Failures in EndoDocument32 pagesSuccess& Failures in Endorasagna reddyNo ratings yet
- All Dental AnatomyDocument114 pagesAll Dental AnatomyKhanh NguyễnNo ratings yet
- Pontic SeminarDocument40 pagesPontic Seminarankita sethiNo ratings yet
- Biological Considerations of Maxillary Denture Foundation AreaDocument40 pagesBiological Considerations of Maxillary Denture Foundation AreaLeena Johnson0% (1)
- Teeth Eruption WordDocument24 pagesTeeth Eruption WordAhmed hegazyNo ratings yet
- Adel Lecture 7&8 Post Crown Part1Document0 pagesAdel Lecture 7&8 Post Crown Part1Ravik FidayatikaNo ratings yet
- Preventive OrthodonticsDocument14 pagesPreventive OrthodonticsVaisakh Ramachandran0% (1)
- Dr. Samahi's lecture on post-insertion denture problems and follow-up visitsDocument10 pagesDr. Samahi's lecture on post-insertion denture problems and follow-up visitsRahul MahajanNo ratings yet
- Radiography Techniques and Safety in Pediatric Dental PatientsDocument125 pagesRadiography Techniques and Safety in Pediatric Dental PatientsHebah NawafNo ratings yet
- Cleft Lip, Cleft Palate and Maxillary Sinus' AkashDocument63 pagesCleft Lip, Cleft Palate and Maxillary Sinus' AkashAkash RautNo ratings yet
- Intro to Fixed Partial DenturesDocument5 pagesIntro to Fixed Partial DenturesThesdave SinghNo ratings yet
- Relationship Between Pendulum Swings and String LengthDocument7 pagesRelationship Between Pendulum Swings and String LengthSULIANI DANNYNo ratings yet
- Non Cervical Lesions Meena MamDocument120 pagesNon Cervical Lesions Meena Mamanshida v pNo ratings yet
- Esthetic Anterior RestorationDocument34 pagesEsthetic Anterior RestorationsandsirameshNo ratings yet
- Lec1 - Bridge (Fixed Partial DentureDocument9 pagesLec1 - Bridge (Fixed Partial Dentureكاظم عبد الحسينNo ratings yet
- Classification Based On TechniqueDocument66 pagesClassification Based On TechniquePranshu Mathur100% (1)
- Resin Bonded Bridge Retention and AdvantagesDocument89 pagesResin Bonded Bridge Retention and AdvantagesNam BuiNo ratings yet
- Cavitypreparation 130320103634 Phpapp01Document60 pagesCavitypreparation 130320103634 Phpapp01Sumit BediNo ratings yet
- Self-ligating brackets do not increase orthodontic treatment efficiencyDocument22 pagesSelf-ligating brackets do not increase orthodontic treatment efficiencyAnkit ChaurhaNo ratings yet
- Amalgam Restoration Failures: Causes and TreatmentsDocument17 pagesAmalgam Restoration Failures: Causes and TreatmentsHaidy Mahmoud El-Sanosy0% (1)
- Methods of Gaining Space 2012 - 2Document3 pagesMethods of Gaining Space 2012 - 2Ahmad KhaledNo ratings yet
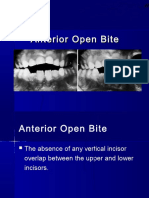
- Dr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentDocument34 pagesDr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentAbdullah100% (1)
- DR Nick Lekic - Space MaintainersDocument35 pagesDR Nick Lekic - Space MaintainersanatomimanusiaNo ratings yet
- Dental Inlay and Onlay Board Exam QuestionsDocument6 pagesDental Inlay and Onlay Board Exam QuestionsErika PanganNo ratings yet
- RCSI Dentistry PG 118 125 A Manual For Space Analysis in The Mixed DentitionDocument8 pagesRCSI Dentistry PG 118 125 A Manual For Space Analysis in The Mixed DentitionkarimelmestekawyNo ratings yet
- Dental BiochemistryDocument17 pagesDental BiochemistryBokiNo ratings yet
- Treatment For ChildrenDocument66 pagesTreatment For ChildrenMohsin HabibNo ratings yet
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 pagesSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCNo ratings yet
- Armamentariums and Its Recent Advances in Dentistry FinalDocument50 pagesArmamentariums and Its Recent Advances in Dentistry FinalOlayiwolaElishaOpeyemiNo ratings yet
- Fixed Partial DentureDocument2 pagesFixed Partial DentureGabriel Chua PaderonNo ratings yet
- Cracked Tooth Syndrome: Presented by Syed - Khaja Ali Uddin M.SC.D (Endo)Document62 pagesCracked Tooth Syndrome: Presented by Syed - Khaja Ali Uddin M.SC.D (Endo)Ali Syed67% (3)
- A History of Dentistry from the most Ancient Times until the end of the Eighteenth CenturyFrom EverandA History of Dentistry from the most Ancient Times until the end of the Eighteenth CenturyNo ratings yet
- High quality CPR improves survival chancesDocument8 pagesHigh quality CPR improves survival chancesSalil Choudhary100% (1)
- High quality CPR improves survival chancesDocument8 pagesHigh quality CPR improves survival chancesSalil Choudhary100% (1)
- Billing Project ReportDocument178 pagesBilling Project ReportSalil ChoudharyNo ratings yet
- Six Sigma DissertationDocument206 pagesSix Sigma DissertationSalil ChoudharyNo ratings yet
- Prefeasbility Report For Setting Up of Diagnostic Center at GulbargaDocument59 pagesPrefeasbility Report For Setting Up of Diagnostic Center at GulbargaSherry SanchesNo ratings yet
- Mha After Bds A Carrier OptionDocument5 pagesMha After Bds A Carrier OptionSalil Choudhary0% (1)
- Mini SAP ProjectDocument6 pagesMini SAP ProjectSalil ChoudharyNo ratings yet
- Cover & Table of ContentsDocument9 pagesCover & Table of ContentsСергей КирстаNo ratings yet
- Gold Alloys PPT SSDocument16 pagesGold Alloys PPT SSSalil Choudhary0% (1)
- Surgicalexposureof Impactedteeth: Pamela L. AlbertoDocument10 pagesSurgicalexposureof Impactedteeth: Pamela L. AlbertoYsabel GutierrezNo ratings yet
- RCSI-Dentistry-Dent Update 2012 EctopicDocument5 pagesRCSI-Dentistry-Dent Update 2012 EctopickarimelmestekawyNo ratings yet
- Mechanics For Gummy Smile CorrectionDocument20 pagesMechanics For Gummy Smile Correctionsandeep kumar senguptaNo ratings yet
- Treatment PlanningDocument12 pagesTreatment PlanningFernaz Behlim100% (1)
- Day 2 Unicorn 1 1Document48 pagesDay 2 Unicorn 1 1Nancy NaeimNo ratings yet
- Theories of Tooth Eruption-For ShahidDocument8 pagesTheories of Tooth Eruption-For Shahidhajar4933No ratings yet
- A To Z Orthodontics Vol 3 Malocclusion1Document36 pagesA To Z Orthodontics Vol 3 Malocclusion1Ishtiaq HasanNo ratings yet
- Payne 1973 Sheep Goat MandibulaDocument24 pagesPayne 1973 Sheep Goat MandibulaSidra ZahoorNo ratings yet
- Use of Lip BumpersDocument21 pagesUse of Lip BumpersDr. Amir MoradiNo ratings yet
- Cleft Lip and Palate Management From Birth To AdulDocument26 pagesCleft Lip and Palate Management From Birth To AdulMelnic FlorentinaNo ratings yet
- Etiology of MalocclusionDocument28 pagesEtiology of MalocclusionPriyaancaHaarsh100% (3)
- Molar Protraction and Uprighting (2 Molar Protraction in The 1 Molar Missing Site and Uprighting An Impacted 3 Molar) PDFDocument7 pagesMolar Protraction and Uprighting (2 Molar Protraction in The 1 Molar Missing Site and Uprighting An Impacted 3 Molar) PDF아미나No ratings yet
- Positional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewDocument10 pagesPositional Guidelines For Orthodontic Mini-Implant Placement in The Anterior Alveolar Region Systematic ReviewLarry MolinaNo ratings yet
- Pediatric OrthodonticsDocument6 pagesPediatric OrthodonticsJaimin PatelNo ratings yet
- Mcintyre Orthodontic Update Canine Part 1Document10 pagesMcintyre Orthodontic Update Canine Part 1Carlos MikaelNo ratings yet
- Deciduous Dentition: Greta Keršytė OF 3 Group Lithuanian University of Health Sciences 2016Document37 pagesDeciduous Dentition: Greta Keršytė OF 3 Group Lithuanian University of Health Sciences 2016GretaKeršytėNo ratings yet
- Permanent Tooth Eruption Based On Chronological Age and Gender in 6-12-Year Old Children On MaduraDocument5 pagesPermanent Tooth Eruption Based On Chronological Age and Gender in 6-12-Year Old Children On MaduraZiyan MalikNo ratings yet
- Does Mandibular Third Molar Have An Impact On Dental Mandibular Anterior Crowding A Literature ReviewDocument4 pagesDoes Mandibular Third Molar Have An Impact On Dental Mandibular Anterior Crowding A Literature ReviewAndrésAcostaNo ratings yet
- Sindrome de Dientes Cortos Sthepen ChuDocument11 pagesSindrome de Dientes Cortos Sthepen Chujorefe12No ratings yet
- Bookshelf NBK401552Document24 pagesBookshelf NBK401552Hanina mamiNo ratings yet
- Impacted Upper Canines by AlmuzianDocument29 pagesImpacted Upper Canines by AlmuzianOctavian TaviNo ratings yet
- Jaypee Gold Standard Mini Atlas Series OrthodonticsDocument158 pagesJaypee Gold Standard Mini Atlas Series OrthodonticsGerardo Gabriel Rodríguez Montalvo89% (9)
- Management of Missing Teeth KokichDocument6 pagesManagement of Missing Teeth KokichTaufiqurrahman Abdul DjabbarNo ratings yet
- Age of The Normal OcclusionDocument8 pagesAge of The Normal OcclusionPaulinaNo ratings yet
- Second Molars ExtractionDocument13 pagesSecond Molars ExtractionSyed Mohammad Osama AhsanNo ratings yet
- Anatomy of Primary Teeth: Dr. Asad Rafique MemonDocument23 pagesAnatomy of Primary Teeth: Dr. Asad Rafique Memonshahzeb memonNo ratings yet