You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Emotions Essential Oils, 2ndDocument86 pagesEmotions Essential Oils, 2ndcatalin86% (7)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Roles of B Vitamins & Their CoenzymesDocument17 pagesRoles of B Vitamins & Their CoenzymesJoyVee Pillagara-De LeonNo ratings yet
- BleedingDocument8 pagesBleedingJoyVee Pillagara-De LeonNo ratings yet
- 10 Nutritional Guidelines For FilipinosDocument5 pages10 Nutritional Guidelines For FilipinosJoyVee Pillagara-De Leon100% (1)
- CaseDocument2 pagesCaseJoyVee Pillagara-De LeonNo ratings yet
- NCP HypokalemiaDocument2 pagesNCP HypokalemiaJoyVee Pillagara-De Leon40% (5)
- 123facts.comDocument12 pages123facts.comJoyVee Pillagara-De LeonNo ratings yet
- SARS Symptoms, Causes, Treatment & DietDocument1 pageSARS Symptoms, Causes, Treatment & DietJoyVee Pillagara-De LeonNo ratings yet
- What Is IsoimmunizationDocument3 pagesWhat Is IsoimmunizationJoyVee Pillagara-De LeonNo ratings yet
- Skew NessDocument5 pagesSkew NessJoyVee Pillagara-De LeonNo ratings yet
- Sars - Is A Life Threatening Viral Respiratory Foods AllowedDocument1 pageSars - Is A Life Threatening Viral Respiratory Foods AllowedJoyVee Pillagara-De LeonNo ratings yet
- DrugsDocument10 pagesDrugsJoyVee Pillagara-De LeonNo ratings yet
- Factors Affecting SolubilityDocument6 pagesFactors Affecting SolubilityJoyVee Pillagara-De LeonNo ratings yet
- Psychiatric NursingDocument89 pagesPsychiatric NursingJoyVee Pillagara-De LeonNo ratings yet
- Psycho Social Theories and Therapy.Document172 pagesPsycho Social Theories and Therapy.JoyVee Pillagara-De LeonNo ratings yet
- CAD plaque builds in arteries causes chest painDocument3 pagesCAD plaque builds in arteries causes chest painJoyVee Pillagara-De LeonNo ratings yet
- PsychopharmacologyDocument11 pagesPsychopharmacologyKristine Joie Danan100% (4)
- What Is IsoimmunizationDocument3 pagesWhat Is IsoimmunizationJoyVee Pillagara-De LeonNo ratings yet
- Nasal PolypsDocument3 pagesNasal PolypsJoyVee Pillagara-De LeonNo ratings yet
- Hematology Is A Screening Test Used To Diagnose and Manage Numerous Disease, It Can Reflect Problems With FluidDocument12 pagesHematology Is A Screening Test Used To Diagnose and Manage Numerous Disease, It Can Reflect Problems With FluidJoyVee Pillagara-De LeonNo ratings yet
- Therapeutic DietDocument7 pagesTherapeutic DietJoyVee Pillagara-De LeonNo ratings yet
- Clear Liquid Diet: PurposeDocument10 pagesClear Liquid Diet: PurposeJoyVee Pillagara-De LeonNo ratings yet
- Psychiatric NursingDocument89 pagesPsychiatric NursingJoyVee Pillagara-De LeonNo ratings yet
- SARSDocument2 pagesSARSJoyVee Pillagara-De Leon100% (1)
- Dengue FeverDocument2 pagesDengue FeverJoyVee Pillagara-De LeonNo ratings yet
- NCP HypokalemiaDocument2 pagesNCP HypokalemiaJoyVee Pillagara-De Leon40% (5)
- CHNDocument14 pagesCHNJoyVee Pillagara-De LeonNo ratings yet
- Menier's DiseaseDocument2 pagesMenier's DiseaseJoyVee Pillagara-De LeonNo ratings yet
- DSM-IV Schizophrenia Types and AssessmentDocument32 pagesDSM-IV Schizophrenia Types and AssessmentJoyVee Pillagara-De LeonNo ratings yet
- Community Health NursingDocument268 pagesCommunity Health NursingNiyad Uthinattu PareethNo ratings yet
- BracesDocument5 pagesBracesJoyVee Pillagara-De LeonNo ratings yet
- SG-3 ProfEd 107Document9 pagesSG-3 ProfEd 107Russel dea EspirituNo ratings yet
- A Case Study of Generalized Anxiety DisorderDocument10 pagesA Case Study of Generalized Anxiety DisorderRina PerezNo ratings yet
- Cross-Cultural Conflict AdjustmentDocument27 pagesCross-Cultural Conflict Adjustmenttapdew 25No ratings yet
- Gaurang - Reportory LectureDocument42 pagesGaurang - Reportory LectureJayakrishnaNo ratings yet
- Chapter V SummaryDocument6 pagesChapter V SummaryCelestine RamosNo ratings yet
- The Role of Pragmatic Competence in Second Language Acquisition PDFDocument137 pagesThe Role of Pragmatic Competence in Second Language Acquisition PDFAnda RascanuNo ratings yet
- Assessment and Behavioral Treatment of Selective MutismDocument22 pagesAssessment and Behavioral Treatment of Selective MutismAdriana ChertiNo ratings yet
- HyperventilationDocument1 pageHyperventilationLim Xin YingNo ratings yet
- Counselling Goals and StagesDocument11 pagesCounselling Goals and StagesPranav Sharma100% (4)
- Fundamentals of Nursin Final Examination-Answer Keys (March 18,2013Document13 pagesFundamentals of Nursin Final Examination-Answer Keys (March 18,2013marsan12No ratings yet
- PSPA3714 Chapter 6 2021Document59 pagesPSPA3714 Chapter 6 2021Kamogelo Makhura100% (1)
- Subiecte Bac 2010Document4 pagesSubiecte Bac 2010unutulmazNo ratings yet
- An Adolescent Case With Internet Addiction and Hacking PDFDocument2 pagesAn Adolescent Case With Internet Addiction and Hacking PDFBaidac Valentin AlexandruNo ratings yet
- Afternoon of An American BoyDocument3 pagesAfternoon of An American Boyaliyahakhan21No ratings yet
- Menopause EIDocument20 pagesMenopause EIZarqa WaseemNo ratings yet
- Expository Essay (English III)Document2 pagesExpository Essay (English III)Faiqa MalikNo ratings yet
- Pediatric MassageDocument12 pagesPediatric MassageFebryLasantiNo ratings yet
- Correlational study between social media use and stress levelsDocument26 pagesCorrelational study between social media use and stress levelsQueen ZaportizaNo ratings yet
- Social media addiction causes and effectsDocument36 pagesSocial media addiction causes and effectsMa. Cheska Kaye BendalNo ratings yet
- Gongora2019 - Neurobiological Evidences Functional and Emotional Aspects Associated With The AmygdalaDocument18 pagesGongora2019 - Neurobiological Evidences Functional and Emotional Aspects Associated With The AmygdalaErick SolisNo ratings yet
- المحاضرة الرابعة نفسيةDocument4 pagesالمحاضرة الرابعة نفسيةTawfek RedaNo ratings yet
- Drug & Alcohol Awareness Employee TrainingDocument59 pagesDrug & Alcohol Awareness Employee TrainingRaymond M. LacsonNo ratings yet
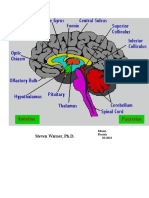
- Sts Cheat Sheet of The BrainDocument30 pagesSts Cheat Sheet of The BrainRahula RakeshNo ratings yet
- THE Center: Anxiety DisordersDocument13 pagesTHE Center: Anxiety DisordersOti VuraNo ratings yet
- Predictive Homeopathy Course Review, Part I: Susanne Saltzman, MDDocument5 pagesPredictive Homeopathy Course Review, Part I: Susanne Saltzman, MDdr TotoNo ratings yet
- Setting Goals in CounsellingDocument4 pagesSetting Goals in CounsellingbinduannNo ratings yet
- Maintaining Team Health and Wellness in This PandemicDocument42 pagesMaintaining Team Health and Wellness in This Pandemicerikka june forosueloNo ratings yet
- Argumentative Essay - NotesDocument15 pagesArgumentative Essay - Notesablanguages94% (18)
- Making Sense of Sensory BehaviourDocument20 pagesMaking Sense of Sensory BehaviourASNo ratings yet