You might also like
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Overview Antenatal CareDocument54 pagesOverview Antenatal CareRizky Dwidya AmirtasariNo ratings yet
- Family PlanningDocument13 pagesFamily PlanningYana PotNo ratings yet
- Prenatal CareDocument32 pagesPrenatal Careyhanne100% (54)
- 2 - Antenatal CareDocument44 pages2 - Antenatal CareJordanBangot50% (2)
- Antenatal CareDocument46 pagesAntenatal CareMarnie MarianieNo ratings yet
- Antenatal CareDocument33 pagesAntenatal CareKamran Afzal100% (1)
- Diagnosis of PregnancyDocument26 pagesDiagnosis of PregnancyMounikaNo ratings yet
- Infections During PregnancyDocument9 pagesInfections During PregnancyKarina Madriaga100% (4)
- Infant FeedingDocument38 pagesInfant Feedinghannanyusof100% (1)
- Prenatal Care by Connie Sussan AustenDocument31 pagesPrenatal Care by Connie Sussan AustenNoraNo ratings yet
- Ps of LaborDocument28 pagesPs of LaborErvina Luisa Delias CampusNo ratings yet
- Obstetric ExamDocument194 pagesObstetric ExamHimmz100% (1)
- CPM16TH Intrapartum and Immediate Postpartum CareDocument25 pagesCPM16TH Intrapartum and Immediate Postpartum CarespringdingNo ratings yet
- A Child With WheezeDocument53 pagesA Child With WheezeCodillia CheongNo ratings yet
- Antenatal CareDocument39 pagesAntenatal CareGAURAV100% (1)
- Obstetric ExaminationDocument26 pagesObstetric Examinationshofa nur rahmannisaNo ratings yet
- Perinatal and Neonatal MortalityDocument40 pagesPerinatal and Neonatal MortalityDuncan Jackson0% (1)
- Antenatal Principles of Antenatal Care 2017Document60 pagesAntenatal Principles of Antenatal Care 2017JanielWright100% (3)
- Premature Rupture of MembranesDocument100 pagesPremature Rupture of Membranesztvill100% (1)
- Aau, Management Guideline On Gyn-ObsDocument202 pagesAau, Management Guideline On Gyn-ObsNaol Abdi100% (10)
- 02 Gestational Trophoblastic DiseaseDocument8 pages02 Gestational Trophoblastic Diseasemisakichan FrandoNo ratings yet
- Obstetrics & Gyn II PDF Abnormal PDFDocument305 pagesObstetrics & Gyn II PDF Abnormal PDFmaezu100% (3)
- Antenatal CareDocument29 pagesAntenatal CareAsti Yuliadha100% (3)
- Amniotic Fluid ColorsDocument2 pagesAmniotic Fluid ColorsgeejeiNo ratings yet
- Menstrual Cycle Lecture NotesDocument23 pagesMenstrual Cycle Lecture Notespmkobar461250% (2)
- Revision Long Case Obs GynaeDocument10 pagesRevision Long Case Obs GynaeHo Yong WaiNo ratings yet
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Assessment of Fetal WellbeingDocument71 pagesAssessment of Fetal WellbeingDanny Apw100% (2)
- HIV in Pregnancy TopicDocument50 pagesHIV in Pregnancy TopicstepnemoNo ratings yet
- Breast FeedingDocument52 pagesBreast Feeding071263galina100% (1)
- Pre Natal Care Book BasedDocument9 pagesPre Natal Care Book BasedAngelaTrinidadNo ratings yet
- Fetal Monitoring Orientation Day-1Document50 pagesFetal Monitoring Orientation Day-1Scott CalfeeNo ratings yet
- Prelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3Document12 pagesPrelabor Rupture of Membranes (Prom) : By-Aditi Grover Roll No. - 3San SiddzNo ratings yet
- Cases in ObgDocument41 pagesCases in ObgShriyansh Chahar0% (1)
- Maternal ExamDocument11 pagesMaternal ExamCherry Mae JasoNo ratings yet
- AbortionDocument35 pagesAbortionZahida Aida Ida Paramore100% (1)
- Normal & Abnormal LabourDocument5 pagesNormal & Abnormal Labourra100% (1)
- Operative ObstetricsDocument4 pagesOperative Obstetricssarguss14100% (3)
- Breech PresentationDocument40 pagesBreech PresentationShuhada Wahab100% (3)
- National Guidelines For Quality Obstetrics and Perinatal Care PDFDocument410 pagesNational Guidelines For Quality Obstetrics and Perinatal Care PDFduncan100% (1)
- Physiology of MenstruationDocument52 pagesPhysiology of Menstruationmahirad001100% (2)
- Diseases Affecting Pregnancy: (Tuberculosis & STD)Document64 pagesDiseases Affecting Pregnancy: (Tuberculosis & STD)Cyrelle Jen TorresNo ratings yet
- PuerperiumDocument85 pagesPuerperiumHema MaliniNo ratings yet
- ObstetricsDocument55 pagesObstetricsKristine Alejandro100% (1)
- Breast Problems After DeviveryDocument19 pagesBreast Problems After DeviverySanthosh.S.UNo ratings yet
- Exam 1 Midterm Study Guide OBDocument23 pagesExam 1 Midterm Study Guide OBAnnissaLarnardNo ratings yet
- Developmental MilestonesDocument52 pagesDevelopmental MilestonesSillmark BacasonNo ratings yet
- Management of Third and Fourth Degree TearsDocument4 pagesManagement of Third and Fourth Degree TearsYwagar YwagarNo ratings yet
- 62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseDocument69 pages62 Lecture Menstrual Cycle Abnormalities, Infertility, MenopauseTarek TarekNo ratings yet
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرNo ratings yet
- Meconium AspirationDocument23 pagesMeconium AspirationWitneyGraceNo ratings yet
- Growth ChartDocument31 pagesGrowth ChartAnand gowda100% (2)
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Abnormal Fetus Presentations: D.R Thomas MutanikwaDocument40 pagesAbnormal Fetus Presentations: D.R Thomas Mutanikwaguidance100% (1)
- Final Ob ChecklistDocument21 pagesFinal Ob ChecklistAlbino Fulgencio Santos III100% (1)
- Family Planning MethodsDocument20 pagesFamily Planning MethodsRoel Marcial100% (2)
- Obstetrics MnemonicsDocument9 pagesObstetrics MnemonicsJared Khoo Er Hau100% (2)
- Antenatal Care AduanaDocument36 pagesAntenatal Care AduanalaarnieNo ratings yet
- Midwifery NursingDocument96 pagesMidwifery NursingMATTHEW KIRARITNo ratings yet
- Practies Test ThreeDocument25 pagesPracties Test ThreeDrSabah LotfyNo ratings yet
- STT520-420: Biostatistics Analysis Dr. Cuixian ChenDocument38 pagesSTT520-420: Biostatistics Analysis Dr. Cuixian ChenDrSabah LotfyNo ratings yet
- Azza Ibrahim Abd El-KaderDocument5 pagesAzza Ibrahim Abd El-KaderDrSabah LotfyNo ratings yet
- LabsDocument114 pagesLabsDrSabah LotfyNo ratings yet
- PPSC MCDRM and Education in Time of PandemicsDocument37 pagesPPSC MCDRM and Education in Time of PandemicsFrederick Deldacan100% (1)
- SmokingDocument116 pagesSmokingyuy21No ratings yet
- CertificateDocument1 pageCertificateManohar NMNo ratings yet
- q3 - Week1 - Health 10 - Study ConceptDocument2 pagesq3 - Week1 - Health 10 - Study ConceptDhess Mulleda MantalaNo ratings yet
- Mapeh PPT ReportingDocument13 pagesMapeh PPT ReportingLoraine Anne Ko0% (1)
- Boil Water AdvisoryDocument2 pagesBoil Water AdvisoryWmar WebNo ratings yet
- Clinical Practice Guidelines in The Evaluation and Management of PCAPDocument38 pagesClinical Practice Guidelines in The Evaluation and Management of PCAPJames de Jesus86% (7)
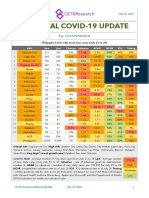
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Community Acquired Pneumonia in Malaysia PDFDocument2 pagesCommunity Acquired Pneumonia in Malaysia PDFCassNo ratings yet
- Guyabano Plant ResearchDocument2 pagesGuyabano Plant ResearchAnnie OmlangNo ratings yet
- Inglês Clara IscedDocument6 pagesInglês Clara IscedCélio PrimeiroNo ratings yet
- Increased Age-Adjusted Cancer Mortality After The 3rd mRNA-Lipid Nanoparticle Vaccine Dose During The COVID-19 Pandemic in JapanDocument14 pagesIncreased Age-Adjusted Cancer Mortality After The 3rd mRNA-Lipid Nanoparticle Vaccine Dose During The COVID-19 Pandemic in JapandanielnagaseNo ratings yet
- Resume For FulbrightDocument5 pagesResume For Fulbrightmango chaunsaNo ratings yet
- Family Problem List: Total: 3.6Document3 pagesFamily Problem List: Total: 3.6wendyNo ratings yet
- Principles of Community Psychology - Toc .Forward - Preface.intro .Refs .IndexesDocument84 pagesPrinciples of Community Psychology - Toc .Forward - Preface.intro .Refs .IndexesAditya Putra KurniawanNo ratings yet
- Leptospirosis FactsDocument1 pageLeptospirosis FactsZenitha FauziaNo ratings yet
- Ex Part 1 Blueprinting Grid NewDocument1 pageEx Part 1 Blueprinting Grid NewKaushika KalaiNo ratings yet
- (Osborn) Chapter 20: Learning Outcomes (Number and Title)Document26 pages(Osborn) Chapter 20: Learning Outcomes (Number and Title)KittiesNo ratings yet
- CHC - 2Document15 pagesCHC - 2Babita Dhruw75% (4)
- Preventive MedicineDocument5 pagesPreventive Medicinescribdnotes123No ratings yet
- Latest Statistics On England Mortality Data Suggest Systematic Mis-Categorisation of Vaccine Status and Uncertain Effectiveness of Covid-19Document24 pagesLatest Statistics On England Mortality Data Suggest Systematic Mis-Categorisation of Vaccine Status and Uncertain Effectiveness of Covid-19RudolfGerNo ratings yet
- Iraqi Injury Surveillance System Annual Report 2013Document46 pagesIraqi Injury Surveillance System Annual Report 2013bejarhasanNo ratings yet
- Avion FluDocument1 pageAvion FluImaan RiazNo ratings yet
- Wesleyan University-Philippines Mabini Extension, Cabanatuan City College of Nursing and Allied Medical Sciences Vision: MissionDocument10 pagesWesleyan University-Philippines Mabini Extension, Cabanatuan City College of Nursing and Allied Medical Sciences Vision: MissionCarissa De Luzuriaga-BalariaNo ratings yet
- Iodine Deficiency Disorder ProgrameDocument26 pagesIodine Deficiency Disorder ProgrameMonalisha SinghNo ratings yet
- HIV in Colombia: An Epidemiologic Point of ViewDocument8 pagesHIV in Colombia: An Epidemiologic Point of ViewJuanJoseHerreraBerrioNo ratings yet
- Maternal Child Nursing Care in Canada 1st Edition Perry Test BankDocument8 pagesMaternal Child Nursing Care in Canada 1st Edition Perry Test BankqocaxNo ratings yet
- Session 11 - A HygieneDocument3 pagesSession 11 - A Hygieneelisabeth hutaurukNo ratings yet
- Adolecent Pregnancy, Elderly Primigravida, Grand Multipara IntroductionDocument3 pagesAdolecent Pregnancy, Elderly Primigravida, Grand Multipara IntroductionmercyNo ratings yet
- Table 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenDocument11 pagesTable 2: Summary of WHO Position Papers - Recommended Routine Immunizations For ChildrenNehaNo ratings yet
- You Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherFrom EverandYou Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherNo ratings yet
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeFrom EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeRating: 3.5 out of 5 stars3.5/5 (13)
- The House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedFrom EverandThe House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedRating: 4.5 out of 5 stars4.5/5 (5)
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeFrom EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo ratings yet
- What to Expect When You’re Expecting (5th Edition)From EverandWhat to Expect When You’re Expecting (5th Edition)Rating: 5 out of 5 stars5/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayFrom EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayRating: 4.5 out of 5 stars4.5/5 (3)
- The Importance of Being Earnest: Classic Tales EditionFrom EverandThe Importance of Being Earnest: Classic Tales EditionRating: 4.5 out of 5 stars4.5/5 (44)
- Natural Hospital Birth: The Best of Both WorldsFrom EverandNatural Hospital Birth: The Best of Both WorldsRating: 5 out of 5 stars5/5 (33)
- The Inimitable Jeeves [Classic Tales Edition]From EverandThe Inimitable Jeeves [Classic Tales Edition]Rating: 5 out of 5 stars5/5 (3)
- Labor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodFrom EverandLabor with Hope: Gospel Meditations on Pregnancy, Childbirth, and MotherhoodRating: 4.5 out of 5 stars4.5/5 (28)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondFrom EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondRating: 4.5 out of 5 stars4.5/5 (39)
- Crones Don't Whine: Concentrated Wisdom for Juicy WomenFrom EverandCrones Don't Whine: Concentrated Wisdom for Juicy WomenRating: 2.5 out of 5 stars2.5/5 (3)
- Awakening Fertility: The Essential Art of Preparing for PregnancyFrom EverandAwakening Fertility: The Essential Art of Preparing for PregnancyRating: 4.5 out of 5 stars4.5/5 (36)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodFrom EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodRating: 5 out of 5 stars5/5 (33)
- ADHD Women: A Holistic Approach To ADHD ManagementFrom EverandADHD Women: A Holistic Approach To ADHD ManagementRating: 5 out of 5 stars5/5 (4)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenFrom EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenRating: 4 out of 5 stars4/5 (154)
- The Comedians in Cars Getting Coffee BookFrom EverandThe Comedians in Cars Getting Coffee BookRating: 4.5 out of 5 stars4.5/5 (8)