You might also like
- All Anzca Primary SAQs With Answers CroppedDocument41 pagesAll Anzca Primary SAQs With Answers CroppedSarah Ip100% (2)
- CRQs and SBAs for the Final FRCA: Questions and detailed answersFrom EverandCRQs and SBAs for the Final FRCA: Questions and detailed answersNo ratings yet
- EMAC Course Handbook V2 3 July 2018Document13 pagesEMAC Course Handbook V2 3 July 2018bobbykrish0% (1)
- Complications of Spinal and Epidural AnesthesiaDocument45 pagesComplications of Spinal and Epidural AnesthesiashikhaNo ratings yet
- Obestetrics GynecologyDocument203 pagesObestetrics GynecologySwamynadh Gandhi ReddiNo ratings yet
- Hot Topics Final JESDocument41 pagesHot Topics Final JESbobbykrishNo ratings yet
- ANZCA MCQs 07-10Document85 pagesANZCA MCQs 07-10Chee_Yeow_6172100% (1)
- BASIC Exam Blueprint PDFDocument3 pagesBASIC Exam Blueprint PDFmichael100% (1)
- Graphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaFrom EverandGraphic Anaesthesia, second edition: Essential diagrams, equations and tables for anaesthesiaNo ratings yet
- Fundamentals of Anaesthesia and QBase Anesthesia 6Document2 pagesFundamentals of Anaesthesia and QBase Anesthesia 6Ch AhmedNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Biggs Medicine, SurgeryDocument19 pagesBiggs Medicine, Surgerymary20149No ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaAnonymous 4jkFIRalKNo ratings yet
- Conduct of AnaesthesiaDocument30 pagesConduct of AnaesthesiaAnirban PalNo ratings yet
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- Mcai CRQ Osce Nov 2021Document15 pagesMcai CRQ Osce Nov 2021Frostz WongNo ratings yet
- Preparation For The Final FRCA 2014 Update1 PDFDocument4 pagesPreparation For The Final FRCA 2014 Update1 PDFSuhas Kapse0% (1)
- Report On The Constructed Response Question / Short Answer Question Paper - September 2019Document6 pagesReport On The Constructed Response Question / Short Answer Question Paper - September 2019cr7No ratings yet
- ANZCA Primary Physiology QuestionsDocument34 pagesANZCA Primary Physiology Questionspriyavirdi100% (1)
- @anesthesia Books 2011 PracticalDocument254 pages@anesthesia Books 2011 PracticalSuci RamadhaniKhairiNo ratings yet
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Physiology 20 21 22Document2 pages1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Physiology 20 21 22rkNo ratings yet
- Anesthesia For Bariatric SurgeryDocument47 pagesAnesthesia For Bariatric Surgerydkhiloi100% (1)
- QBase Anaesthesia 1 PDFDocument209 pagesQBase Anaesthesia 1 PDFmarceloNo ratings yet
- Race 2019Document418 pagesRace 2019Sadia KhanNo ratings yet
- 4 5796434682396543760Document289 pages4 5796434682396543760Jhe CaselNo ratings yet
- Kate Laver's Primary FRCA Guide: My Revision (For Exam in June)Document3 pagesKate Laver's Primary FRCA Guide: My Revision (For Exam in June)M H DuNo ratings yet
- Management of High Spinal AnesthesiaDocument8 pagesManagement of High Spinal AnesthesiaYeni TriastutikNo ratings yet
- Fred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008Document53 pagesFred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008lmjeksoreNo ratings yet
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- Stats For FRCADocument5 pagesStats For FRCAPhil BlackieNo ratings yet
- Basic Science For AnaesthetistsDocument224 pagesBasic Science For AnaesthetistsciccioNo ratings yet
- Exm Sba July2012 PDFDocument5 pagesExm Sba July2012 PDFSuhas KapseNo ratings yet
- Physics and Anesthesia Final ReportDocument148 pagesPhysics and Anesthesia Final ReportGerald Caesar O. LibrandaNo ratings yet
- ANESTHESIA-Pediatrics Airway SyndromesDocument12 pagesANESTHESIA-Pediatrics Airway SyndromeshollyuNo ratings yet
- Anaesthesia Explained PDFDocument22 pagesAnaesthesia Explained PDFaksinu100% (1)
- Total Revision For The Primary Frca 2nd EditionDocument53 pagesTotal Revision For The Primary Frca 2nd Editionizwan taufikNo ratings yet
- A Primer For The Primary FANZCA ExaminationDocument62 pagesA Primer For The Primary FANZCA ExaminationAnnie100% (1)
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Anaesthesia On The MoveDocument244 pagesAnaesthesia On The MoveLucas ArenasNo ratings yet
- AnaesthesiaDocument44 pagesAnaesthesiamadmaxmaxmus50% (2)
- Physics of Anaesthesia Made Easy: Review ArticleDocument7 pagesPhysics of Anaesthesia Made Easy: Review ArticleEinstein A. MustafaNo ratings yet
- Anesthesia Resident Requirements PDFDocument21 pagesAnesthesia Resident Requirements PDFJulieNo ratings yet
- @anesthesia Books 2018 GuidelinesDocument16 pages@anesthesia Books 2018 GuidelinesAgil Rumboko SumitroNo ratings yet
- Thsesis TopicsDocument17 pagesThsesis Topicsvvb_frndNo ratings yet
- Primary FRCA - OSCEs in Anaesthesia (PDFDrive)Document310 pagesPrimary FRCA - OSCEs in Anaesthesia (PDFDrive)Manuela CormioNo ratings yet
- The Hong Kong College of Anaesthesiologists Final Fellowship Examination July/September 2007 Examiners ReportDocument16 pagesThe Hong Kong College of Anaesthesiologists Final Fellowship Examination July/September 2007 Examiners ReportJane KoNo ratings yet
- Diploma Guide - EnglishDocument11 pagesDiploma Guide - EnglishAndra Victoria TitaNo ratings yet
- HintsfortheAnesthesiologyBoardExaminationRev1 6Document98 pagesHintsfortheAnesthesiologyBoardExaminationRev1 6cooloffyouNo ratings yet
- Royal College X AnesthesiaDocument66 pagesRoyal College X AnesthesiaManuela CormioNo ratings yet
- QBase Anaesthesia 4 (1st 1998)Document178 pagesQBase Anaesthesia 4 (1st 1998)Supriya Patil100% (3)
- Primary FRCA MCQ Guide UpdateDocument21 pagesPrimary FRCA MCQ Guide UpdatePriya VetrivelNo ratings yet
- FRCA Primary Basic ScienceDocument14 pagesFRCA Primary Basic ScienceAbdelrahman MamdouhNo ratings yet
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- Pedi AnesthsiaDocument192 pagesPedi AnesthsiaHarish BhatNo ratings yet
- Update EmergenciesDocument84 pagesUpdate EmergenciesElaineNo ratings yet
- Evidence-Based Obstetric AnesthesiaFrom EverandEvidence-Based Obstetric AnesthesiaStephen H. HalpernNo ratings yet
- Pediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderFrom EverandPediatric Anesthesia: A Guide for the Non-Pediatric Anesthesia ProviderNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- PBL 1 - Post Streptococcal Rheumatic Fever PolicyDocument8 pagesPBL 1 - Post Streptococcal Rheumatic Fever PolicyAinur AbdrakhmanovaNo ratings yet
- Nursing Management HydrocephalusDocument4 pagesNursing Management HydrocephalusPrecious Mae Benologa100% (1)
- ProspectusDocument156 pagesProspectusNareshNo ratings yet
- Anxiety Disorders BBDocument18 pagesAnxiety Disorders BBRyan Justin BoudreauxNo ratings yet
- Jordan University of Science and TechnologyDocument33 pagesJordan University of Science and TechnologyNourAldin AbuSalehNo ratings yet
- The Letter of Intent To Enter PracticeDocument4 pagesThe Letter of Intent To Enter Practicekazniels100% (1)
- World Congress Integrative Medicine & Health 2017: Part OneDocument64 pagesWorld Congress Integrative Medicine & Health 2017: Part OneGabrielAbarcaNo ratings yet
- ADR Form PDFDocument2 pagesADR Form PDFCha Tuban DianaNo ratings yet
- Negative Effects of Video GamesDocument5 pagesNegative Effects of Video GamesMadeNo ratings yet
- Gpat 2019Document51 pagesGpat 2019Nishabh KushwahaNo ratings yet
- Retinos PDFDocument83 pagesRetinos PDFPaulo Gan100% (2)
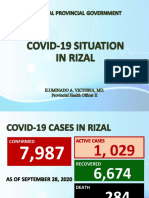
- Covid19 Situation in RizalDocument23 pagesCovid19 Situation in RizalToni Quitalig GamezNo ratings yet
- The ConjungtivaDocument111 pagesThe ConjungtivaLuvita Amallia SyadhatinNo ratings yet
- SPC Marbonor 100 MLDocument6 pagesSPC Marbonor 100 MLJelena TerzicNo ratings yet
- Visual NeglectDocument2 pagesVisual NeglectPierre A. RodulfoNo ratings yet
- Dabur PresentationDocument26 pagesDabur PresentationShraddha Khurana100% (1)
- Compare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenDocument12 pagesCompare Prokaryotes and Eukaryotes: Gram +ve Gram - Ve Peptidoglycan Layer Teichoic Acid Surface AntigenAamir BugtiNo ratings yet
- Drug InteractionsDocument21 pagesDrug InteractionsPawan Deshmukh100% (1)
- Health Policy Memo MgenoviaDocument5 pagesHealth Policy Memo Mgenoviaapi-302138606No ratings yet
- Interpretation of Weld RadiographsDocument10 pagesInterpretation of Weld RadiographsarianaseriNo ratings yet
- Resume PortfolioDocument1 pageResume Portfolioapi-386291240No ratings yet
- VibhorDocument21 pagesVibhorNeha ShuklaNo ratings yet
- Reliance Policy Extn Request FormDocument1 pageReliance Policy Extn Request Formanshu_204No ratings yet
- Theraputic UltrasoundDocument64 pagesTheraputic UltrasoundRoshni KhanNo ratings yet
- QuestionaireDocument3 pagesQuestionaireEking InNo ratings yet
- IMCI Chart BookletDocument66 pagesIMCI Chart Bookletnorwin_033875No ratings yet
- CyberTherapy & Rehabilitation, Issue 3 (3), Winter 2010.Document52 pagesCyberTherapy & Rehabilitation, Issue 3 (3), Winter 2010.Giuseppe RivaNo ratings yet
- 2023 Welcome Event SOPDocument13 pages2023 Welcome Event SOPNur Adila Binti AzmanNo ratings yet
- Surgeon-Performed Ultrasound As A Diagnostic Tool in AppendicitisDocument6 pagesSurgeon-Performed Ultrasound As A Diagnostic Tool in Appendicitisansar ahmedNo ratings yet