You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Gothic Voodoo in Africa and HaitiDocument19 pagesGothic Voodoo in Africa and HaitiJames BayhylleNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Horizon Trial: Witness Statement in Support of Recusal ApplicationDocument12 pagesHorizon Trial: Witness Statement in Support of Recusal ApplicationNick Wallis100% (1)
- Text and Meaning in Stanley FishDocument5 pagesText and Meaning in Stanley FishparthNo ratings yet
- Digest Pre TrialDocument2 pagesDigest Pre TrialJei Essa AlmiasNo ratings yet
- Computer Engineering Project TopicsDocument5 pagesComputer Engineering Project Topicskelvin carterNo ratings yet
- I'M NOT A SKET - I Just Grew Up With Them (Chapter 4 & 5)Document13 pagesI'M NOT A SKET - I Just Grew Up With Them (Chapter 4 & 5)Chantel100% (3)
- PRIMER - CFC Young Couples ProgramDocument3 pagesPRIMER - CFC Young Couples Programgeorgeskie8100% (2)
- La Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Document36 pagesLa Mujer Ante El COVID-19: Retos y Oportunidades para La Salud y El Sector Salud.Presentaciones_FKNo ratings yet
- Closing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesDocument39 pagesClosing The Cancer Divide & Strengthening Health Systems: Interwoven OpportunitiesPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief.Document37 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief.Presentaciones_FKNo ratings yet
- Closing The Cancer DivideDocument36 pagesClosing The Cancer DividePresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoverageDocument36 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief: An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Breast Cancer in The AmericasDocument27 pagesBreast Cancer in The AmericasPresentaciones_FKNo ratings yet
- Closing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsDocument39 pagesClosing The Cancer Divide For Women in The Americas: Diagonal Health System InnovationsPresentaciones_FKNo ratings yet
- Valuing To InvaluableDocument24 pagesValuing To InvaluablePresentaciones_FKNo ratings yet
- Closing The Cancer Divide: Lessons From Women's HealthDocument43 pagesClosing The Cancer Divide: Lessons From Women's HealthPresentaciones_FKNo ratings yet
- Valuing To Invaluable. Contributions of Women To Health and Health SectorDocument26 pagesValuing To Invaluable. Contributions of Women To Health and Health SectorPresentaciones_FKNo ratings yet
- Alleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoverageDocument16 pagesAlleviating The Access Abyss in Palliative Care and Pain Relief-An Imperative of Universal Health CoveragePresentaciones_FKNo ratings yet
- Strengthening Health Systems: Learning From CancerDocument33 pagesStrengthening Health Systems: Learning From CancerPresentaciones_FKNo ratings yet
- Closing The Cancer DivideDocument40 pagesClosing The Cancer DividePresentaciones_FKNo ratings yet
- Closing Divides: Global Health Challenges and OpportunitiesDocument26 pagesClosing Divides: Global Health Challenges and OpportunitiesPresentaciones_FKNo ratings yet
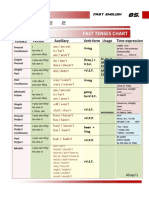
- Table 2: Fast Tenses ChartDocument5 pagesTable 2: Fast Tenses ChartAngel Julian HernandezNo ratings yet
- International Law Detailed Notes For Css 2018Document95 pagesInternational Law Detailed Notes For Css 2018Tooba Hassan Zaidi100% (1)
- Linking Social Science Theories/Models To EducationDocument2 pagesLinking Social Science Theories/Models To EducationAlexa GandioncoNo ratings yet
- Uwamungu Et Al 2022 - Contaminacion de Suelos Por MicroplasticosDocument14 pagesUwamungu Et Al 2022 - Contaminacion de Suelos Por MicroplasticosXXUHAJNo ratings yet
- Impacts of Cultural Differences On Project SuccessDocument10 pagesImpacts of Cultural Differences On Project SuccessMichael OlaleyeNo ratings yet
- Full Download Fundamentals of Thermodynamics 6th Edition Sonntag Solutions ManualDocument20 pagesFull Download Fundamentals of Thermodynamics 6th Edition Sonntag Solutions Manualadenose.helveo0mvl100% (39)
- Farhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoDocument32 pagesFarhat Ziadeh - Winds Blow Where Ships Do Not Wish To GoabshlimonNo ratings yet
- Persephone and The PomegranateDocument3 pagesPersephone and The PomegranateLíviaNo ratings yet
- Channarapayttana LandDocument8 pagesChannarapayttana Landnagaraja.raj.1189No ratings yet
- Practice Test 01 - Part ADocument9 pagesPractice Test 01 - Part AJose David Pascacio GrandaNo ratings yet
- DIS Investment ReportDocument1 pageDIS Investment ReportHyperNo ratings yet
- Specific Relief Act, 1963Document23 pagesSpecific Relief Act, 1963Saahiel Sharrma0% (1)
- Deed OfAdjudication Cresencio Abuluyan BasilioDocument4 pagesDeed OfAdjudication Cresencio Abuluyan BasilioJose BonifacioNo ratings yet
- 09 Task Performance 1-ARG - ZABALA GROUPDocument6 pages09 Task Performance 1-ARG - ZABALA GROUPKylle Justin ZabalaNo ratings yet
- Baseball Stadium Financing SummaryDocument1 pageBaseball Stadium Financing SummarypotomacstreetNo ratings yet
- NEERJA 7th April 2016 Pre Shoot Draft PDFDocument120 pagesNEERJA 7th April 2016 Pre Shoot Draft PDFMuhammad Amir ShafiqNo ratings yet
- People Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JDocument10 pagesPeople Vs Gonzales-Flores - 138535-38 - April 19, 2001 - JTrexPutiNo ratings yet
- Satisfaction On Localized Services: A Basis of The Citizen-Driven Priority Action PlanDocument9 pagesSatisfaction On Localized Services: A Basis of The Citizen-Driven Priority Action PlanMary Rose Bragais OgayonNo ratings yet
- Project Initiation & Pre-StudyDocument36 pagesProject Initiation & Pre-StudyTuấn Nam NguyễnNo ratings yet
- Anglais OverconsumptionDocument3 pagesAnglais OverconsumptionAnas HoussiniNo ratings yet
- Unit 2 Organisational CultureDocument28 pagesUnit 2 Organisational CultureJesica MaryNo ratings yet
- Annaphpapp 01Document3 pagesAnnaphpapp 01anujhanda29No ratings yet
- Romanian Architectural Wooden Cultural Heritage - TheDocument6 pagesRomanian Architectural Wooden Cultural Heritage - ThewoodcultherNo ratings yet