You might also like
- Management of Developing DentitionDocument51 pagesManagement of Developing Dentitionahmed alshaariNo ratings yet
- Fractured Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFractured Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- THE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSFrom EverandTHE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSNo ratings yet
- Serial ExtractionDocument23 pagesSerial ExtractionBindu VincentNo ratings yet
- MalocclusionDocument95 pagesMalocclusionsonal agarwalNo ratings yet
- Malocclusion OrthoDocument79 pagesMalocclusion OrthoFourthMolar.com100% (2)
- 275 AnchorageDocument41 pages275 AnchorageMohan NathNo ratings yet
- Development of Dentition and Occlusion: Sujina.SDocument214 pagesDevelopment of Dentition and Occlusion: Sujina.SsathyaNo ratings yet
- Jaw Deformity Treatment MethodsDocument62 pagesJaw Deformity Treatment MethodsCarmen Vizarro RodriguezNo ratings yet
- Role of Orthodontist in Cleft Lip & Palate TreatmentDocument125 pagesRole of Orthodontist in Cleft Lip & Palate TreatmentNiyati VerulkarNo ratings yet
- Simple Tooth Extraction Technique: Amin AbusallamahDocument35 pagesSimple Tooth Extraction Technique: Amin AbusallamahThiagoDaher100% (1)
- Basic Principles of GrowthDocument29 pagesBasic Principles of GrowthMohsin HabibNo ratings yet
- Impacted Maxillary CanineDocument8 pagesImpacted Maxillary CanineMatin Ahmad Khan100% (1)
- Goals of Orthodontic TreatmentDocument14 pagesGoals of Orthodontic TreatmentemanNo ratings yet
- Canine ImpactionDocument31 pagesCanine Impactionavanthika krishnarajNo ratings yet
- Impacted Teeth RemovalDocument35 pagesImpacted Teeth RemovalChaitanya SuramNo ratings yet
- Final Impacted Third Molars-1Document62 pagesFinal Impacted Third Molars-1Anam ShaikhNo ratings yet
- Classification of Malloclusion1Document19 pagesClassification of Malloclusion1Shashank Kapadia100% (1)
- Methods of Gaining Space 1. / Orthodontic Courses by Indian Dental AcademyDocument64 pagesMethods of Gaining Space 1. / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Preventive OrthodonticDocument19 pagesPreventive OrthodonticNada EmadNo ratings yet
- Maxillary molar distalization techniques under 40 charactersDocument8 pagesMaxillary molar distalization techniques under 40 charactersGoutam NookalaNo ratings yet
- Instrument Used in ExodontaDocument32 pagesInstrument Used in ExodontaNoor Abdullah AlNo ratings yet
- Complications of Extraction: Prsenting By: Rahul TiwariDocument75 pagesComplications of Extraction: Prsenting By: Rahul TiwariIrfan AliNo ratings yet
- Bows & RetractorsDocument53 pagesBows & RetractorsSri RengalakshmiNo ratings yet
- Arch ExpansionDocument32 pagesArch ExpansionMoola Bharath Reddy100% (5)
- Risks in Orthodontic TreatmentDocument60 pagesRisks in Orthodontic TreatmentPaRpArOsSaNo ratings yet
- Palatal ExpansionDocument6 pagesPalatal ExpansionAlyssa Garello100% (1)
- 6-Ateiology of MO IIDocument8 pages6-Ateiology of MO IIKhalid Mortaja100% (1)
- Orthopedo AssDocument4 pagesOrthopedo AssIvyRoselleLacasandileCabañeroNo ratings yet
- Development of Dental OcclusionDocument89 pagesDevelopment of Dental OcclusionMothi KrishnaNo ratings yet
- Cleft Lip, Cleft Palate and Maxillary Sinus' AkashDocument63 pagesCleft Lip, Cleft Palate and Maxillary Sinus' AkashAkash RautNo ratings yet
- Mathods of Gaining SpaceDocument22 pagesMathods of Gaining SpaceAamir FaizNo ratings yet
- Complete Denture Prosthodontics in Children With Ectodermal DysplasiaDocument29 pagesComplete Denture Prosthodontics in Children With Ectodermal DysplasiaAmit BhargavNo ratings yet
- PREPROSTHETIC SURGERY - RamonDocument49 pagesPREPROSTHETIC SURGERY - Ramonjamaica faith ramonNo ratings yet
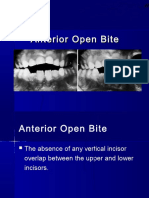
- Open BiteDocument14 pagesOpen Biteفاطمة فالح ضايف مزعلNo ratings yet
- Indirect Bonding: Process, Advantages, and FAQsDocument77 pagesIndirect Bonding: Process, Advantages, and FAQsPruessada DeeyingNo ratings yet
- Classification of MalocclusionDocument79 pagesClassification of MalocclusionMittali Vaibhav Sabnis50% (2)
- Myths of Orthodontic GnathologyDocument9 pagesMyths of Orthodontic GnathologymentacityNo ratings yet
- Serial ExtractionDocument38 pagesSerial Extractionmanishpankaj123No ratings yet
- Development of Dentition & OcclusionDocument109 pagesDevelopment of Dentition & OcclusionSyed Mohammad Osama Ahsan100% (1)
- Class Ii Malocclusion: Usman & MehmoodDocument41 pagesClass Ii Malocclusion: Usman & MehmoodmehmudbhattiNo ratings yet
- OPEN BITE 1 / Orthodontic Courses by Indian Dental AcademyDocument23 pagesOPEN BITE 1 / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Dr. Munizeh Khan S.R OrthodonticsDocument38 pagesDr. Munizeh Khan S.R OrthodonticsMohsin HabibNo ratings yet
- Etiology of Malocclusion & Habits: Dr. Biswaroop MohantyDocument74 pagesEtiology of Malocclusion & Habits: Dr. Biswaroop MohantynehanoopurNo ratings yet
- Retention and Relapse DR Shabeel PNDocument33 pagesRetention and Relapse DR Shabeel PNShabeel Pn100% (2)
- Molares InclinadosDocument13 pagesMolares Inclinadosmaria jose peña rojas100% (1)
- ARCH EXPANSIONDocument33 pagesARCH EXPANSIONGareth BaleNo ratings yet
- Dr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentDocument34 pagesDr. Hla Hla Yee Discusses Anterior Open Bite and Deep Bite TreatmentAbdullah100% (1)
- Royal London Space AnalysisDocument47 pagesRoyal London Space AnalysisYusra ShaukatNo ratings yet
- Developmental DisordersDocument36 pagesDevelopmental DisordersANJINo ratings yet
- TMD Examination and TreatmentDocument65 pagesTMD Examination and Treatmentdr666No ratings yet
- 5-Aetiology of MalocclusionDocument7 pages5-Aetiology of MalocclusionKhalid Mortaja100% (1)
- The Midline Diagnosis and Treatment ARTUROCAMACHODocument10 pagesThe Midline Diagnosis and Treatment ARTUROCAMACHOMiguel AngelNo ratings yet
- Bond FailureDocument3 pagesBond Failuredentist97No ratings yet
- Non XNDocument9 pagesNon XNNaveenNo ratings yet
- Preventive OrthodonticsDocument14 pagesPreventive OrthodonticsVaisakh Ramachandran0% (1)
- Orthodontic Indices OverviewDocument10 pagesOrthodontic Indices OverviewBhavikPatelNo ratings yet
- Surgically Assisted Rapid Maxillary Expansion Combined With MaxillaryDocument21 pagesSurgically Assisted Rapid Maxillary Expansion Combined With MaxillaryKumar NiwalikarNo ratings yet
- A Study of History by ToynbeeDocument580 pagesA Study of History by ToynbeeMohsin Habib100% (10)
- 12 Pin Retained RestorationDocument59 pages12 Pin Retained RestorationMohsin HabibNo ratings yet
- Implants Prostheses Treatment Planning 30 Jan 2012Document48 pagesImplants Prostheses Treatment Planning 30 Jan 2012Mohsin HabibNo ratings yet
- Impacted Teeth Part BDocument18 pagesImpacted Teeth Part BMohsin HabibNo ratings yet
- TMPD 5Document28 pagesTMPD 5Mohsin HabibNo ratings yet
- Implants Prostheses Jan 2012Document168 pagesImplants Prostheses Jan 2012Mohsin Habib100% (1)
- Trigeminal Neuralgia (Tic Douloureux)Document49 pagesTrigeminal Neuralgia (Tic Douloureux)Mohsin HabibNo ratings yet
- Infections of Oro Facial & Neck Region ADocument68 pagesInfections of Oro Facial & Neck Region AMohsin HabibNo ratings yet
- Class 2. Trismus, ClassificationDocument18 pagesClass 2. Trismus, ClassificationMohsin Habib100% (1)
- Infections of Oro Facial & Neck Region BDocument39 pagesInfections of Oro Facial & Neck Region BMohsin Habib100% (1)
- AAA RPD 004 A Support A by DR GHANIDocument14 pagesAAA RPD 004 A Support A by DR GHANIMohsin HabibNo ratings yet
- Cysts of JawsDocument36 pagesCysts of JawsMohsin HabibNo ratings yet
- Material For ImplantDocument24 pagesMaterial For ImplantMohsin HabibNo ratings yet
- Ntroduction To Operative DentistryDocument55 pagesNtroduction To Operative DentistryMohsin HabibNo ratings yet
- TMJ Anatomy 1Document19 pagesTMJ Anatomy 1Mohsin HabibNo ratings yet
- ExodoniaDocument184 pagesExodoniaMohsin HabibNo ratings yet
- Fixed Partial Dentures 2Document153 pagesFixed Partial Dentures 2Mohsin Habib100% (1)
- Effects of Dental Implant Length and BoneDocument6 pagesEffects of Dental Implant Length and BoneMohsin HabibNo ratings yet
- Impacted Teeth Part BDocument18 pagesImpacted Teeth Part BMohsin HabibNo ratings yet
- Medoralv 13 I 2 P 124Document5 pagesMedoralv 13 I 2 P 124Mohsin HabibNo ratings yet
- DR Fabio RossiDocument3 pagesDR Fabio RossiMohsin Habib100% (1)
- Selection of Optimal Dental Implant Diameter and Length in Type IV Bone 3dfeaDocument7 pagesSelection of Optimal Dental Implant Diameter and Length in Type IV Bone 3dfeaMohsin HabibNo ratings yet
- Dental Implants MaterialsDocument10 pagesDental Implants MaterialsMohsin HabibNo ratings yet
- Impacted Teeth Part ADocument27 pagesImpacted Teeth Part AMohsin HabibNo ratings yet
- Bio Materials (IMPLANT)Document33 pagesBio Materials (IMPLANT)Mohsin HabibNo ratings yet
- DR Shuja PresentationDocument54 pagesDR Shuja PresentationMohsin HabibNo ratings yet
- Impacted Teeth Part CDocument34 pagesImpacted Teeth Part CMohsin HabibNo ratings yet
- Cysts of JawsDocument36 pagesCysts of JawsMohsin HabibNo ratings yet
- 8.1. Complete DentureDocument42 pages8.1. Complete DentureMohsin HabibNo ratings yet
- Healthcare System of PakistanDocument4 pagesHealthcare System of PakistanIJARP PublicationsNo ratings yet
- The Challenges of Effective Communication Between Health Information Officers and PatientsDocument5 pagesThe Challenges of Effective Communication Between Health Information Officers and Patientshassan mamudNo ratings yet
- Hospital Name N AddDocument38 pagesHospital Name N AddShruti AgrawalNo ratings yet
- TRANSMISSION OF HEMOPHILIA: A SEX-LINKED GENETIC DISORDERDocument4 pagesTRANSMISSION OF HEMOPHILIA: A SEX-LINKED GENETIC DISORDERlady ann apple colipanoNo ratings yet
- Barriers of Communication Between Nurse and CheldreenDocument22 pagesBarriers of Communication Between Nurse and CheldreenOmArio KhayiNo ratings yet
- Lect15&16 Fluids&ElectrolytesDocument77 pagesLect15&16 Fluids&Electrolyteskhurram na100% (1)
- 2008 CPC Practice Exam Section 1 AnswersDocument12 pages2008 CPC Practice Exam Section 1 AnswersBeverly GraciousNo ratings yet
- Perioperatif Nursing PDFDocument93 pagesPerioperatif Nursing PDFNurvanny HusnaNo ratings yet
- Sansbury Resume PDFDocument2 pagesSansbury Resume PDFapi-502971487No ratings yet
- Reaction PaperDocument3 pagesReaction Paperedmond callenNo ratings yet
- Wound Essentials 5 How To Choose The Appropriate Dressing For Each Wound TypeDocument4 pagesWound Essentials 5 How To Choose The Appropriate Dressing For Each Wound TypeJacqueline MilonNo ratings yet
- MSBOS1Document29 pagesMSBOS1elenaa.hp28No ratings yet
- Saying No To PatientsDocument6 pagesSaying No To PatientsCristina SeNo ratings yet
- Perio Notes CombinedDocument71 pagesPerio Notes CombinedHayley WelshNo ratings yet
- World Health Champion Game Questions Ampamp Answers BRMDocument18 pagesWorld Health Champion Game Questions Ampamp Answers BRMSalem alarjaniNo ratings yet
- Turnaround Times of Lab Test UGDDocument4 pagesTurnaround Times of Lab Test UGDdjebrutNo ratings yet
- (Charles H. Adler, J. Eric Ahlskog) Parkinson's DiDocument490 pages(Charles H. Adler, J. Eric Ahlskog) Parkinson's Disteven_mize9147100% (2)
- The Import Ants of Leech in AvurvedaDocument2 pagesThe Import Ants of Leech in AvurvedaDr.saurabh SharmaNo ratings yet
- Anz Complaint ProcessDocument2 pagesAnz Complaint ProcessBung HerryNo ratings yet
- Sunset EyesDocument1 pageSunset EyesBilly Shan LastKagerooboroNo ratings yet
- Dretske, F. 1991, Conscious Acts and Their ObjectsDocument2 pagesDretske, F. 1991, Conscious Acts and Their ObjectskhrinizNo ratings yet
- Pediatric ShockDocument19 pagesPediatric ShockdarlingcarvajalduqueNo ratings yet
- A Doctor Nay, A SaviourDocument3 pagesA Doctor Nay, A Saviourt.prasad.saiNo ratings yet
- Assignment On "Parts of Removable Partial Denture"Document8 pagesAssignment On "Parts of Removable Partial Denture"Jeba Afia JebinNo ratings yet
- Blood Glucose MonitoringDocument10 pagesBlood Glucose MonitoringSarah Jane MaganteNo ratings yet
- Neonatal Pain Assessment &managementDocument14 pagesNeonatal Pain Assessment &managementKhaula BethelNo ratings yet
- Nursing Practice I - Foundation of Professional NursingDocument9 pagesNursing Practice I - Foundation of Professional NursingNeenya SisonNo ratings yet
- Asepsis and Infection Control Nursing SchoolDocument20 pagesAsepsis and Infection Control Nursing Schoolleonardo orozco100% (1)
- Biperiden Drug StudyDocument2 pagesBiperiden Drug StudyMelissa Fatima Laurente Dosdos100% (1)
- Working of Blood BanksDocument146 pagesWorking of Blood BanksRupali Vaiti100% (1)