You might also like
- Nursing Prioritization of The Patient Ne PDFDocument13 pagesNursing Prioritization of The Patient Ne PDFBambim TexonNo ratings yet
- Reflection About Palliative Care and End of Life CareDocument5 pagesReflection About Palliative Care and End of Life CareVILLEJO JHOVIALENNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Providing Culturally Appropriate Care: A Literature ReviewDocument9 pagesProviding Culturally Appropriate Care: A Literature ReviewLynette Pearce100% (1)
- Cardiopulmonary Assessment and InterventionDocument51 pagesCardiopulmonary Assessment and InterventionPreciousShaizNo ratings yet
- Ethical Dilemmas in Nursing PDFDocument5 pagesEthical Dilemmas in Nursing PDFtitiNo ratings yet
- Little Schmidy Falls Risk AssessmentDocument1 pageLittle Schmidy Falls Risk AssessmentrenystrawberryNo ratings yet
- Observation Summary 2Document5 pagesObservation Summary 2api-493028287No ratings yet
- Supervising Registered Nurse: Passbooks Study GuideFrom EverandSupervising Registered Nurse: Passbooks Study GuideNo ratings yet
- OWL at Purdue University Printable Handouts Using American Psychological Association (APA) FormatDocument28 pagesOWL at Purdue University Printable Handouts Using American Psychological Association (APA) Formatrryan100% (3)
- FinalintegrativereviewDocument17 pagesFinalintegrativereviewapi-346349076No ratings yet
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideFrom EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideNo ratings yet
- Navigating Long-Term Care - A Practical Approach for NursesFrom EverandNavigating Long-Term Care - A Practical Approach for NursesNo ratings yet
- Ethical Problems in Nursing ManagementDocument4 pagesEthical Problems in Nursing ManagementJen Rhae LimNo ratings yet
- Caring at The End of Life - Approaching Death - NCBI Bookshelf PDFDocument18 pagesCaring at The End of Life - Approaching Death - NCBI Bookshelf PDFBelaislam Belaulama100% (1)
- Spirituality in Healthcare: Perspectives for Innovative PracticeFrom EverandSpirituality in Healthcare: Perspectives for Innovative PracticeNo ratings yet
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionFrom EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionNo ratings yet
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansDocument11 pagesCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessNo ratings yet
- Assessing AdlDocument7 pagesAssessing AdlFitriana WarliatyNo ratings yet
- The Balance Concept in Health and Nursing: A Universal Approach to Care and SurvivalFrom EverandThe Balance Concept in Health and Nursing: A Universal Approach to Care and SurvivalNo ratings yet
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperFrom EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperNo ratings yet
- Medicaid in Long Term CareDocument7 pagesMedicaid in Long Term Carerara100% (1)
- Achieving Cultural Competency: A Case-Based Approach to Training Health ProfessionalsFrom EverandAchieving Cultural Competency: A Case-Based Approach to Training Health ProfessionalsNo ratings yet
- AMSN Scope Standards MS NursingDocument27 pagesAMSN Scope Standards MS NursingPaulEspartinezNo ratings yet
- Improving The Quality of Care in An Acute Care Facility Through RDocument88 pagesImproving The Quality of Care in An Acute Care Facility Through RNor-aine Salazar AccoyNo ratings yet
- Bedside Shift Report and Utilizing The EhrDocument9 pagesBedside Shift Report and Utilizing The Ehrapi-349480325No ratings yet
- Culture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewDocument49 pagesCulture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewAlberto JaramilloNo ratings yet
- Registered Professional Nurse: Passbooks Study GuideFrom EverandRegistered Professional Nurse: Passbooks Study GuideNo ratings yet
- Palliative Care Guidelines-20 November2013Document69 pagesPalliative Care Guidelines-20 November2013Olga ŢiuNo ratings yet
- American Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideDocument20 pagesAmerican Nurses Credentialing Center (ANCC) Adult Nurse Practitioner Exam Study GuideMcRee Learning CenterNo ratings yet
- Trainin On Compassionate, Respectful and Caring Health ProfessionalsDocument21 pagesTrainin On Compassionate, Respectful and Caring Health ProfessionalsnibretzwNo ratings yet
- Nurse's Assistant NotesDocument3 pagesNurse's Assistant NotesLonefallen DarkNo ratings yet
- Sample PSW Resume - 3Document2 pagesSample PSW Resume - 3branislava1301No ratings yet
- The Slim Book of Health Pearls: Hormones, Nerves, and StressFrom EverandThe Slim Book of Health Pearls: Hormones, Nerves, and StressNo ratings yet
- Chapter 26Document46 pagesChapter 26meeeenonNo ratings yet
- Research in Palliative Care PresentationDocument20 pagesResearch in Palliative Care PresentationNICKY SAMBONo ratings yet
- Transition to the Registered Professional Nurse Role: Passbooks Study GuideFrom EverandTransition to the Registered Professional Nurse Role: Passbooks Study GuideNo ratings yet
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- 1 Emotional Labor and Organizational Emotional CareDocument29 pages1 Emotional Labor and Organizational Emotional CareCarola GonzálezNo ratings yet
- Health Information Technology A Complete Guide - 2020 EditionFrom EverandHealth Information Technology A Complete Guide - 2020 EditionNo ratings yet
- Health Record Technician I: Passbooks Study GuideFrom EverandHealth Record Technician I: Passbooks Study GuideNo ratings yet
- Govt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeDocument17 pagesGovt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeMamta YadavNo ratings yet
- Safety Unfolding Nursing Case StudyDocument3 pagesSafety Unfolding Nursing Case StudyclarimerNo ratings yet
- Legal Implications Document A Schneider PDFDocument52 pagesLegal Implications Document A Schneider PDFAmrod Inglorion100% (2)
- Cellulitis in Adults - Guideline Flowchart Hospital in The Home Guideline For Management at HomeDocument2 pagesCellulitis in Adults - Guideline Flowchart Hospital in The Home Guideline For Management at HomeAnonymous 4txA8N8etNo ratings yet
- Crtitical Care Nursing: Imran Yousafzai BSN, MSPH, PGHRHM, Mhpe Lecturer KMUDocument42 pagesCrtitical Care Nursing: Imran Yousafzai BSN, MSPH, PGHRHM, Mhpe Lecturer KMUikram ullah khanNo ratings yet
- 1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)Document39 pages1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)NTRisforthinkersNo ratings yet
- Restraint Use and Patient Care: Nnual CompetencyDocument35 pagesRestraint Use and Patient Care: Nnual CompetencyrustiejadeNo ratings yet
- Pilot Project ReportDocument26 pagesPilot Project ReportInclusionNorthNo ratings yet
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-508132058No ratings yet
- How to Succeed New Graduate Nursing Job Interview & Bachelor of Nursing Clinical Placement?From EverandHow to Succeed New Graduate Nursing Job Interview & Bachelor of Nursing Clinical Placement?No ratings yet
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationDocument8 pagesDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonNo ratings yet
- NCM101 Health Assessment ExaminationDocument11 pagesNCM101 Health Assessment ExaminationJonah R. Merano100% (1)
- HEENT (Head, Eyes, Ear, Nose & Throat) : Pupils. The Pupils Are in The Center of TheDocument2 pagesHEENT (Head, Eyes, Ear, Nose & Throat) : Pupils. The Pupils Are in The Center of TheJonah R. MeranoNo ratings yet
- Assessment and History of The Head and NeckDocument6 pagesAssessment and History of The Head and NeckJonah R. MeranoNo ratings yet
- Assessment - of - SKIN HAIR AND NAILS CHECKLISTDocument8 pagesAssessment - of - SKIN HAIR AND NAILS CHECKLISTJonah R. MeranoNo ratings yet
- Assessment of Heart - CHECKLISTDocument3 pagesAssessment of Heart - CHECKLISTJonah R. MeranoNo ratings yet
- Assessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEDocument27 pagesAssessment of The Heart-Neck Vessels-Peripheral Vessels-PULSEJonah R. MeranoNo ratings yet
- MindsetDocument1 pageMindsetJonah R. MeranoNo ratings yet
- Assessment - of - SKIN HAIR AND NAILS CHECKLISTDocument8 pagesAssessment - of - SKIN HAIR AND NAILS CHECKLISTJonah R. MeranoNo ratings yet
- Introduction To Physical ExaminationDocument18 pagesIntroduction To Physical ExaminationJonah R. MeranoNo ratings yet
- QRLE ChecklistDocument2 pagesQRLE ChecklistJonah R. MeranoNo ratings yet
- CS - Drug Study - TactisDocument2 pagesCS - Drug Study - TactisJonah R. MeranoNo ratings yet
- End of Life Issue (JC)Document15 pagesEnd of Life Issue (JC)Jonah R. MeranoNo ratings yet
- HEENT Exam Teaching DocketDocument10 pagesHEENT Exam Teaching DocketJonah R. MeranoNo ratings yet
- Change ModelDocument23 pagesChange ModelJonah R. MeranoNo ratings yet
- Learning Through Experience FinalDocument60 pagesLearning Through Experience FinalJonah R. MeranoNo ratings yet
- Care of The DyingDocument4 pagesCare of The Dyingprokuno89% (9)
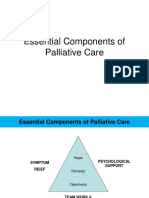
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano50% (4)
- Curriculum DevelopmentDocument20 pagesCurriculum DevelopmentWilfred NiloberNo ratings yet
- Fundamentals of BioethicsDocument14 pagesFundamentals of BioethicsJonah R. MeranoNo ratings yet
- Aesthetic NursingDocument12 pagesAesthetic NursingJonah R. MeranoNo ratings yet
- Bench BookDocument1 pageBench BookJonah R. MeranoNo ratings yet
- Bench BookDocument1 pageBench BookJonah R. MeranoNo ratings yet
- Taxonomy of CognitiveDocument3 pagesTaxonomy of CognitiveJonah R. MeranoNo ratings yet
- History of Hospice CareDocument72 pagesHistory of Hospice CareJonah R. MeranoNo ratings yet
- Scaling Up Community-DrivenDocument43 pagesScaling Up Community-DrivenJonah R. MeranoNo ratings yet
- What Is CloningDocument9 pagesWhat Is CloningJonah R. MeranoNo ratings yet
- EuthanasiaDocument18 pagesEuthanasiaJonah R. MeranoNo ratings yet
- Ethical ThoughtsDocument39 pagesEthical ThoughtsJonah R. Merano100% (2)
- Artificial InseminationDocument8 pagesArtificial InseminationJonah R. MeranoNo ratings yet
- Taxonomy of CognitiveDocument3 pagesTaxonomy of CognitiveJonah R. MeranoNo ratings yet