You might also like
- Rural Water and Sanitation in UgandaDocument47 pagesRural Water and Sanitation in UgandaDesire IsaiahNo ratings yet
- 4 Report-GhatgaunDocument19 pages4 Report-GhatgaunBipin GyawaliNo ratings yet
- Rift Valley Water Supply and Sanitation ProjectDocument59 pagesRift Valley Water Supply and Sanitation ProjectcherogonyaNo ratings yet
- Project Proposal PPP Water and Sanitation-FinalDocument2 pagesProject Proposal PPP Water and Sanitation-FinalmanjariNo ratings yet
- CED Design Alternatives-1Document38 pagesCED Design Alternatives-1Liban HalakeNo ratings yet
- Water Project Aplication To Global HandDocument7 pagesWater Project Aplication To Global HandLoic NgashiNo ratings yet
- Pictorial Presentation of WASH Activities in Rural KenyaFrom EverandPictorial Presentation of WASH Activities in Rural KenyaRating: 5 out of 5 stars5/5 (1)
- Housing UnderproductionDocument18 pagesHousing UnderproductionCalifornia YIMBYNo ratings yet
- HOYWIK Multi-Purpose CentreDocument14 pagesHOYWIK Multi-Purpose CentreKeneni AbabulguNo ratings yet
- Societal Project ReportDocument28 pagesSocietal Project Reportನಂದನ್ ಎಂ ಗೌಡ100% (2)
- Roadside Service StationDocument34 pagesRoadside Service StationGedeBudiSuprayogaNo ratings yet
- Sanitation Projects EthiopiaDocument39 pagesSanitation Projects EthiopiaAdnan ShaameNo ratings yet
- Part 3.2 Telecom Network Infrastructure PlanningDocument32 pagesPart 3.2 Telecom Network Infrastructure PlanningEithu Thutun0% (1)
- Affordable Access To Adequate Wash FacilitiesDocument23 pagesAffordable Access To Adequate Wash FacilitiesJoseph GichehaNo ratings yet
- Department of Road 2010-13Document32 pagesDepartment of Road 2010-13Ramesh PokharelNo ratings yet
- Zimbabwe - Urgent Water Supply and Sanitation Rehabilitation Project - Phase 2 - Appraisal ReportDocument28 pagesZimbabwe - Urgent Water Supply and Sanitation Rehabilitation Project - Phase 2 - Appraisal ReportTrevor T Paraziva100% (1)
- Toilet Program (Philippines Setting)Document19 pagesToilet Program (Philippines Setting)Nasripha MalawaniNo ratings yet
- MembershipDocument11 pagesMembershipSherif HelmyNo ratings yet
- CAMBODIA: Rural Roads Improvement ProjectDocument20 pagesCAMBODIA: Rural Roads Improvement ProjectADBGADNo ratings yet
- Proposal For Capacity Building of YouthDocument7 pagesProposal For Capacity Building of YouthdennisNo ratings yet
- Mini Project Report - Tus.G3Document10 pagesMini Project Report - Tus.G3mohmmad omar100% (1)
- Sample Project ReportDocument90 pagesSample Project ReporthardcorefsNo ratings yet
- MONITORING AND EVALUATION FOR RESULTS - PSNP Presentation - For Woreda-AdamaDocument47 pagesMONITORING AND EVALUATION FOR RESULTS - PSNP Presentation - For Woreda-AdamaDDE1964100% (1)
- HISM200-1-Course Outline-Jan-Jun2023-SL-V1-02023 PDFDocument79 pagesHISM200-1-Course Outline-Jan-Jun2023-SL-V1-02023 PDFThembisa NobethaNo ratings yet
- 12 Design Speed and Design TrafficDocument34 pages12 Design Speed and Design TrafficMiguel Michael Cahuana QuispeNo ratings yet
- Global Kids Online: Children's Rights in The Digital Age: Inception ReportDocument10 pagesGlobal Kids Online: Children's Rights in The Digital Age: Inception ReportyomnahelmyNo ratings yet
- Public Participation Improvement in Kalmunai Municipal CouncilDocument9 pagesPublic Participation Improvement in Kalmunai Municipal CouncilJowsi Abdul Jabbar100% (1)
- Feasibility Report PMDocument17 pagesFeasibility Report PMpiu_chatterjee100% (1)
- TOR - Distribution of Cooking StovesDocument4 pagesTOR - Distribution of Cooking StovessubxaanalahNo ratings yet
- Tor DMDP 2-DesignDocument96 pagesTor DMDP 2-DesignKitozay94No ratings yet
- Melamchi Water Supply Project - 2011 PDFDocument150 pagesMelamchi Water Supply Project - 2011 PDFSuman AryalNo ratings yet
- Session 1.2C - National Sewerage and Septage Management Program PDFDocument19 pagesSession 1.2C - National Sewerage and Septage Management Program PDFWilbur SuandingNo ratings yet
- The Professional Review: Guideline For ReviewersDocument3 pagesThe Professional Review: Guideline For ReviewersPaul AlcantaraNo ratings yet
- Project Identification ReportDocument269 pagesProject Identification ReportnalakasaNo ratings yet
- Vision Long Island Infrastructure ListDocument33 pagesVision Long Island Infrastructure ListLong Island Business NewsNo ratings yet
- Project 5 - Residential HomesDocument44 pagesProject 5 - Residential HomesFrancis John F. LopezNo ratings yet
- 0003 - Password Based Access Control System With Motorized Gate Buzzer and LCD DisplayDocument3 pages0003 - Password Based Access Control System With Motorized Gate Buzzer and LCD DisplayPrasad RaoNo ratings yet
- Project Proposal: Name of Organization: Gram Vikas TrustDocument4 pagesProject Proposal: Name of Organization: Gram Vikas TrustLALA TECHNo ratings yet
- Increasing The Capacities of Cable Cars For Use in Public TransportDocument16 pagesIncreasing The Capacities of Cable Cars For Use in Public TransportPavlos VardoulakisNo ratings yet
- Kartheek D N: ObjectiveDocument2 pagesKartheek D N: ObjectiveArun PeddiNo ratings yet
- The Uganda Institution of Professional Engineers (UIPE)Document18 pagesThe Uganda Institution of Professional Engineers (UIPE)isaacssebulibaNo ratings yet
- Internship Report Projects Have Done DurDocument38 pagesInternship Report Projects Have Done DurfikrueNo ratings yet
- RFP Integrated Parking Management 2Document10 pagesRFP Integrated Parking Management 2amhosny64No ratings yet
- Qcad - QuestionsDocument6 pagesQcad - Questionsjhonsver SALVATIERRA DE LA CRUZNo ratings yet
- Project Proposal On Ongwediva Rural Water SupplyDocument4 pagesProject Proposal On Ongwediva Rural Water SupplyTinaNo ratings yet
- Sample Final Year Thesis SynopsisDocument2 pagesSample Final Year Thesis SynopsisGrad-Dreams Education Consulting Group, Mumbai - India89% (9)
- Project Management Information SystemsDocument5 pagesProject Management Information Systemsمحمد محمود مهديNo ratings yet
- Urban Governance: Topic GuideDocument60 pagesUrban Governance: Topic GuideSaifuddin SidikiNo ratings yet
- The Role of Education in Livelihoods in The Somali Region of EthiopiaDocument132 pagesThe Role of Education in Livelihoods in The Somali Region of EthiopiaFeinstein International CenterNo ratings yet
- Water Supply EngineeringDocument2 pagesWater Supply EngineeringsushilNo ratings yet
- Technical Proposal PDFDocument11 pagesTechnical Proposal PDFEQ13No ratings yet
- Sample Project ReportDocument77 pagesSample Project ReportChavda ashwinNo ratings yet
- Project ProposalDocument14 pagesProject ProposalGimhan GodawatteNo ratings yet
- Design and Analysis of An Institutional BuildingDocument6 pagesDesign and Analysis of An Institutional BuildingdbpublicationsNo ratings yet
- Proposal IncompleteDocument13 pagesProposal Incompletesujan gautam0% (1)
- Water Supply ReportDocument29 pagesWater Supply ReportAyesha UsmanNo ratings yet
- DBF UgandaDocument15 pagesDBF Ugandakumargaurav01No ratings yet
- Swacch Bharat AbhiyaanDocument10 pagesSwacch Bharat AbhiyaanParesh ShrivastavaNo ratings yet
- Feasibility Study Detailed Project Report of Road Safety Advocacy Park at Kanyakumari-End Point PDFDocument214 pagesFeasibility Study Detailed Project Report of Road Safety Advocacy Park at Kanyakumari-End Point PDFsalemmanojNo ratings yet
- PROGRESS REPORT JULY 2020 FinalDocument14 pagesPROGRESS REPORT JULY 2020 FinalOKELLO OKOT PATRICKNo ratings yet
- Innovative Urban Tenure in The Philippines. Challenge, Approaches and Institutionalization. Summary ReportDocument64 pagesInnovative Urban Tenure in The Philippines. Challenge, Approaches and Institutionalization. Summary ReportOswar MungkasaNo ratings yet
- Qualitative Assessment. The Social Impacts of Cash Transfer Programmes in Indonesia. Draft Initial Findings.Document33 pagesQualitative Assessment. The Social Impacts of Cash Transfer Programmes in Indonesia. Draft Initial Findings.Oswar MungkasaNo ratings yet
- Visioning As Participatory Planning ToolDocument98 pagesVisioning As Participatory Planning ToolUnited Nations Human Settlements Programme (UN-HABITAT)No ratings yet
- Fiscal Decentralisation in JapanDocument46 pagesFiscal Decentralisation in JapanUnited Nations Human Settlements Programme (UN-HABITAT)100% (1)
- Join The World Urban Campaign. Better City Better Life.Document24 pagesJoin The World Urban Campaign. Better City Better Life.Oswar MungkasaNo ratings yet
- Urban Planning For City Leaders PDFDocument188 pagesUrban Planning For City Leaders PDFAutif SayyedNo ratings yet
- Training For Hygiene Promotion. Part 1: Essential To KnowDocument56 pagesTraining For Hygiene Promotion. Part 1: Essential To KnowOswar Mungkasa100% (3)
- Training For Hygiene Promotion. Part 2: Useful To KnowDocument40 pagesTraining For Hygiene Promotion. Part 2: Useful To KnowOswar Mungkasa100% (3)
- Public-Private Partnership in Housing and Urban DevelopmentDocument46 pagesPublic-Private Partnership in Housing and Urban DevelopmentUnited Nations Human Settlements Programme (UN-HABITAT)100% (1)
- Green CitiesDocument428 pagesGreen CitiesAsian Development Bank75% (4)
- Islamic Principles and Land. Opportunities For EngagementDocument24 pagesIslamic Principles and Land. Opportunities For EngagementOswar MungkasaNo ratings yet
- Fiscal Decentralization in The PhilippinesDocument56 pagesFiscal Decentralization in The PhilippinesUnited Nations Human Settlements Programme (UN-HABITAT)100% (4)
- Training For Hygiene Promotion. Part 2: Useful To KnowDocument40 pagesTraining For Hygiene Promotion. Part 2: Useful To KnowOswar Mungkasa100% (3)
- Training For Hygiene Promotion. Part 3: Additional Training For HP CoordinatorsDocument64 pagesTraining For Hygiene Promotion. Part 3: Additional Training For HP CoordinatorsOswar Mungkasa100% (1)
- Guidelines For Public Health Promotion in EmergenciesDocument110 pagesGuidelines For Public Health Promotion in EmergenciesOxfam100% (2)
- PHAST (Participatory Hygiene and Sanitation Transformation) For An EmergencyDocument29 pagesPHAST (Participatory Hygiene and Sanitation Transformation) For An EmergencyOswar Mungkasa100% (3)
- Model Guidelines For MAINSTREAMING wATER AND sANITATION eMERGENCIES pROTRACTED cRISES, LRRD and Disaster Preparedness Operations.Document133 pagesModel Guidelines For MAINSTREAMING wATER AND sANITATION eMERGENCIES pROTRACTED cRISES, LRRD and Disaster Preparedness Operations.Oswar Mungkasa100% (1)
- Environmental Health Promotion Capacity Building: A Training Guide Based On CARE'sHygiene Promotion ManualDocument60 pagesEnvironmental Health Promotion Capacity Building: A Training Guide Based On CARE'sHygiene Promotion ManualOswar MungkasaNo ratings yet
- Training For Hygiene Promotors and HP Coordinators. Part 1 of 3. Essential To KnowDocument176 pagesTraining For Hygiene Promotors and HP Coordinators. Part 1 of 3. Essential To KnowOswar Mungkasa100% (1)
- BCC in Emergencies, A ToolkitDocument241 pagesBCC in Emergencies, A ToolkitLisa WoodsNo ratings yet
- Facts For Life 2002Document175 pagesFacts For Life 2002UNICEF SverigeNo ratings yet
- Hygiene Promotion in EmergenciesDocument41 pagesHygiene Promotion in EmergenciesOswar Mungkasa50% (2)
- JMP Drinking Water and Sanitation Report 2012Document66 pagesJMP Drinking Water and Sanitation Report 2012mcm2222No ratings yet
- An Introduction To The Australian Mid-Term Expenditure Framework (MTEF) and Performance Based Budgeting (PBB) REFORMSDocument7 pagesAn Introduction To The Australian Mid-Term Expenditure Framework (MTEF) and Performance Based Budgeting (PBB) REFORMSOswar MungkasaNo ratings yet
- Masterplan of Indonesia Economic ExpansionDocument210 pagesMasterplan of Indonesia Economic ExpansionHenry So E DiarkoNo ratings yet
- WASH Hygiene Promotion. Training For Community MobilisersDocument73 pagesWASH Hygiene Promotion. Training For Community MobilisersOswar Mungkasa83% (6)
- Water Supply in East Asia and The Pacific - 2012 UpdateDocument8 pagesWater Supply in East Asia and The Pacific - 2012 UpdateOswar MungkasaNo ratings yet
- A Snapshot - 2012 Update. Sanitation and Hygiene in East Asia and The PacificDocument10 pagesA Snapshot - 2012 Update. Sanitation and Hygiene in East Asia and The PacificOswar MungkasaNo ratings yet
- Planning Mid-Term Expenditure Framework (MTEF) and Performance Based Budgeting (PBB) Reforms For Next Five Years and BeyondDocument4 pagesPlanning Mid-Term Expenditure Framework (MTEF) and Performance Based Budgeting (PBB) Reforms For Next Five Years and BeyondOswar MungkasaNo ratings yet
- Collimation of Binoculars With A LampDocument33 pagesCollimation of Binoculars With A LampchristianNo ratings yet
- Materi 2 - Obligation, Prohibition, and Suggestion - AdviceDocument12 pagesMateri 2 - Obligation, Prohibition, and Suggestion - AdviceShadrina ChaerunissaNo ratings yet
- Instructional Module: IM No.: IM-NSTP 1-1STSEM-2021-2022Document6 pagesInstructional Module: IM No.: IM-NSTP 1-1STSEM-2021-2022Princess DumlaoNo ratings yet
- Philippine Ecd Checklist Class Summary (Post-Test) SY: 2022-2023Document5 pagesPhilippine Ecd Checklist Class Summary (Post-Test) SY: 2022-2023UltravioletHeartNo ratings yet
- Prompt by NikistDocument4 pagesPrompt by NikistMãnoj MaheshwariNo ratings yet
- What's New: Contemporary Quiz#5Document2 pagesWhat's New: Contemporary Quiz#5Christian Castañeda100% (1)
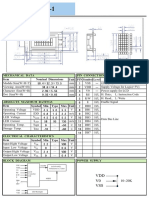
- V0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemDocument1 pageV0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemBasir Ahmad NooriNo ratings yet
- Nursery Car Seat Supplement 2023Document40 pagesNursery Car Seat Supplement 2023doniNo ratings yet
- Guidelines For The Oral Presentation Bands Singers e MusicDocument2 pagesGuidelines For The Oral Presentation Bands Singers e Musicjuliusdelazare100% (1)
- Assessment of Spinach Seedling Health Status and Chlorophyll Content by Multivariate Data Analysis and Multiple Linear Regression of Leaf Image FeaturesDocument9 pagesAssessment of Spinach Seedling Health Status and Chlorophyll Content by Multivariate Data Analysis and Multiple Linear Regression of Leaf Image FeaturesYugal KumarNo ratings yet
- Altium Rigid Flex GuidebookDocument40 pagesAltium Rigid Flex GuidebookKiran Jot Singh100% (1)
- MAS500 2011 Vår Masteroppgave Henrik Engedal Per Magne EgelidDocument130 pagesMAS500 2011 Vår Masteroppgave Henrik Engedal Per Magne EgelidPoppy DanielsNo ratings yet
- Diagram 1 Shows An AbacusDocument11 pagesDiagram 1 Shows An AbacusHema BalasubramaniamNo ratings yet
- Philosophical Warfare and The Shadow of IdeasDocument5 pagesPhilosophical Warfare and The Shadow of IdeasDavid MetcalfeNo ratings yet
- Aashto t87Document3 pagesAashto t87AL Bé NizNo ratings yet
- Summative Test 3.1 Math 10Document2 pagesSummative Test 3.1 Math 10Christian DecenaNo ratings yet
- MUMBAI ConsultantsDocument43 pagesMUMBAI ConsultantsER RaviNo ratings yet
- All I Need Is Love by Klaus Kinski 0394549163 PDFDocument5 pagesAll I Need Is Love by Klaus Kinski 0394549163 PDFFernanda ArzaguetNo ratings yet
- Oo All MethodDocument35 pagesOo All Methodmeeraselvam19761970No ratings yet
- Getting You To Test Day: An 8-Week Prep Plan For The TOEFL TestDocument2 pagesGetting You To Test Day: An 8-Week Prep Plan For The TOEFL Testsmith90No ratings yet
- Czujniki Temperatury MOTOMETERDocument7 pagesCzujniki Temperatury MOTOMETERhelp3rNo ratings yet
- Java ProgrammingDocument134 pagesJava ProgrammingArt LookNo ratings yet
- Frequency Spectrum On XXX OperatorsDocument4 pagesFrequency Spectrum On XXX OperatorsPeng Yuan FengNo ratings yet
- Vocabulary Placement TestDocument3 pagesVocabulary Placement TestMonica Vergara MejiaNo ratings yet
- Control System Engineering: Topic Block Diagram RepresentationDocument24 pagesControl System Engineering: Topic Block Diagram RepresentationWaqas AfzalNo ratings yet
- EPAL TRW EPAL2 2edition Section2 Part2 GBDocument45 pagesEPAL TRW EPAL2 2edition Section2 Part2 GBGabriele AsnaghiNo ratings yet
- Existing VendorsDocument1 pageExisting VendorsSuperintending EngineerNo ratings yet
- DSO Digital Storage Oscilloscope: ApplicationDocument2 pagesDSO Digital Storage Oscilloscope: ApplicationmsequipmentsNo ratings yet
- Multidimensional Flow Modeling of The Compression Test of A Gaede Pump Stage in The Viscous RegimeDocument9 pagesMultidimensional Flow Modeling of The Compression Test of A Gaede Pump Stage in The Viscous RegimeAsif HameedNo ratings yet
- Pests and Diseases Identification in MangoDocument4 pagesPests and Diseases Identification in MangoBaino Olpugad Gerald100% (1)